DR Congo’s cobalt boom carries an unwanted cargo: uranium

On the southern border of the Democratic Republic of Congo, the lumbering
trucks carrying cobalt into Zambia may soon have to pass through towering
radiation detectors — a sign of mounting concerns about uranium
contamination in the ores that are powering the electric revolution.
The DR Congo is the world’s largest producer of cobalt, an essential metal for
batteries. But the frequent presence of radioactive materials at some of
its biggest cobalt mines has led to health risks for workers, rejected
shipments and concerns about safeguarding nuclear material, according to an
investigation by the FT and Lighthouse Reports, a journalism non-profit.
With limited state oversight in mining regions, non-proliferation
specialists and Congolese officials worry that uranium-laced cobalt ore and
other radioactive material could fall into the wrong hands or enter a
covert supply chain hidden from international regulators. Uranium occurs
naturally across the country’s vast “copper belt” region, which
includes the mine that produced the uranium used in the atomic bombs in the
second world war.
New research shows the amount of uranium mingled with the
country’s cobalt exports is much greater than previously believed:
between 2000 and 2024 it was enough to produce 600 nuclear weapons, or fuel
a large 1GW nuclear reactor for a decade, if extracted and enriched.
FT 30th July 2026, https://www.ft.com/content/77815def-6f50-4adf-8ba3-3643de7bf8ab
As Trump boosts nuclear power, regulators seek to eliminate a longstanding radiation safety practice

Count On News 2. by: JENNIFER McDERMOTT, Associated Press, Jul 26, 2026
The Nuclear Regulatory Commission is proposing to eliminate a foundational safety principle that has for 50 years minimized the radiation people in the United States are exposed to and that has been adopted around the world.
Currently, facilities such as nuclear plants, hospitals or academic institutions that use radioactive materials must ensure radiation exposures are kept “as low as reasonably achievable” — the ALARA principle. The NRC proposal would abandon that philosophy while keeping a separate standard on maximum radiation exposure.
The two standards have worked together in radiation safety. Dose limits set the maximum amount of radiation the public and radiation workers can be exposed to, while ALARA kept radiation exposure as low as practical under those limits. Research shows radiation exposure increases a person’s chance of getting cancer, a risk that increases as the dose increases.
The dose limits are not changing. But the NRC, which regulates civilian nuclear energy technologies and radioactive materials, now wants to replace ALARA with a “graded approach” that includes several actions facilities must take depending on the potential dose of radiation to workers. More rigorous radiation protection measures would be required when approaching dose limits to ensure they aren’t exceeded.
This comes as President Donald Trump attempts to quadruple domestic nuclear energy production because of surging electricity demand amid a data center and artificial intelligence boom. Reforming the NRC is one way Trump is trying to speed up nuclear reactor development. He instructed the federal agency in an executive order last year to “ adopt science-based radiation limits.”
The Energy Department, which oversees national energy policies, has already stopped using ALARA. The NRC expects to finalize its radiation protection regulations in the coming months………………………………………………………………………………………….
Without ALARA, could radiation doses creep closer to the limits?…………………………………………………………….
Some experts question the wisdom of eliminating ALARA
Edwin Lyman, director of nuclear power safety at the Union of Concerned Scientists, cautions that some parts of the NRC proposal could raise permissible radiation doses in certain cases, while still staying below the cap. Lyman highlighted a proposed revision to radionuclide emissions standards, in particular.
Radiation exposure to the general public is limited to 100 millirem per year. A typical dose of radiation from a chest X-ray is 10 millirem.
The NRC wants to increase its radionuclide emissions standards from a conservative 10 millirem per year dose to 25 millirem per year, based on a hypothetical person living in a house at the property line for a nuclear plant.
The NRC should improve, rather than eliminate, ALARA, Lyman said, to protect the public and workers. ALARA has become a political target because some people mistakenly believe radiation exposures have to be as low as possible no matter the cost, Lyman said. In reality, it allows tradeoffs………………………………………………………………………………………………………………………… https://www.counton2.com/news/national-news/ap-as-trump-boosts-nuclear-power-regulators-seek-to-eliminate-a-longstanding-radiation-safety-rule/
Hegseth Announces Testosterone Testing as Part of Push for “Lethal” Military
Hegseth has previously told servicemembers that troops will have to meet “the highest male standard.”
, By Chris Walker , Truthout, July 15, 2026
On Wednesday, Secretary of Defense Pete Hegseth announced a new policy aimed at increasing testosterone levels for servicemembers — a move that has been discouraged by health experts.
In a social media post announcing the policy, Hegseth stated that the most “decisive tactical advantage” the U.S. military has “will always be the individual warfighter.”
“We have a sacred duty to maintain that advantage, which is why we must constantly look for new ways to optimize your performance, your resilience, and your long-term health,” the Defense Secretary stated. “To meet that commitment today, I’m authorizing a new screening program for testosterone deficiency for our service members, ensuring you have the right testosterone levels to operate at your absolute best.”
The new policy aims to provide, as part of yearly screening, mandatory testosterone level testing for servicemembers over the age of 30, with those under that age being allowed to request it. Hegseth emphasized that what happens next is up to the individual.
“If treatment is recommended, it’s entirely your choice to receive testosterone replacement therapy,” or TRT, he said.
But the overall message from Hegseth was clear: The military wants and is prioritizing higher testosterone levels in its soldiers.
“The modern battlefield is brutal and unrelenting. It requires and demands maximum psychological and mental readiness, and by addressing these health markers early, we’re keeping you on the leading edge of lethality and giving you the same level of support that you give this nation,” he said.
Hegseth noted that it is “well-established science that as we age, testosterone levels often naturally drop.” While that is true, the “drop” in levels isn’t significant for most people, and certainly not for those of military age — levels drop by about 1 percent per year for people over the age of 30.
While the program appears to be voluntary beyond testing, some servicemembers may feel pressured to take medical supplements after their test results come in (especially since Hegseth’s video message was accompanied by the words, “The High-T Department of War”). Hegseth’s push could also prompt servicemembers to take testosterone supplements before their testing, without proper guidance.
Indeed, Hegseth’s message may feed into the current epidemic of online misinformation, tying masculinity to higher testosterone levels.
“This is a huge problem,” endocrinologist Channa Jayasena, of Imperial College London, told The Guardian in November. “Hospital specialists are seeing patients coming in after having private blood tests, often arranged through influencers, perhaps, and then being told by inexperienced doctors or a wide range of healthcare professionals that they should start testosterone. The advice they are giving is wrong.”
Notably, the Food and Drug Administration (FDA) advises against testosterone replacement therapy unless there is a specific medical reason for it.
Health experts questioned Hegseth’s new initiative.
“I used to do testosterone research — testing for T levels in troops doesn’t make sense without a medical reason,” public health scientist and epidemiologist Eric Feigl-Ding said in a post on X reacting to Hegseth’s announcement. “T level is not associated with higher cognitive function. T can drop because of stress or exhaustion — but TRT doesn’t always improve physical performance.”
The result of TRT is “mixed at best,” Feigl-Ding added.
Testosterone is a naturally occurring sex hormone, commonly associated with being the major hormone for men, though it is present in everyone at varying levels, including women. Benefits of the hormone include increasing muscle size and strength, as well as bone growth.
But according to Harvard Medical School, artificially high levels of testosterone have also been associated with a number of health problems, such as:
- Heart damage and a higher risk of heart attacks;
- High blood pressure and increased cholesterol levels;
- Higher risks for blood clots;
- Liver disease;
- Prostate enlargement;
- Headaches;
- Insomnia, mood swings, irritability, impaired judgment, and possibly overly aggressive behavior.
Hegseth’s announcement came with no similar statement of concern for the health of servicewomen, and is consistent with his past statements on (and apparent obsession with) creating a more “manly” military…………………..https://truthout.org/articles/hegseth-announces-testosterone-testing-as-part-of-push-for-lethal-military/?utm_source=Truthout&utm_campaign=c1d90ce474-EMAIL_CAMPAIGN_2026_07_15_09_13_COPY_01&utm_medium=email&utm_term=0_bbb541a1db-cd76c245dc-650192793
Challenging New York Times’s Suggestion That We Should Stop Worrying and Love Radiation

The 2006 National Academy of Sciences report on Biological Effects of Ionizing Radiation (BEIR VII) substantiates Liner No Threshhold LNT, as did the 2021 NRC decision to deny a 2015 request to get rid of LNT.
Karl Grossman, July 15, 2026 https://fair.org/home/challenging-nyts-suggestion-that-we-should-stop-worrying-and-love-radiation/
Alfred Meyer, long active in Physicians for Social Responsibility and former co-chair of its Radiation and Health Committee, challenged an article in the July 3 New York Times, headlined “US to Overhaul Radiation Safety Rules to Spur Nuclear Expansion.”
In a July 6 letter to the article’s author, Brad Plumer, Meyer wrote:
When I read the New York Times business page, I assume that there is a high level of investigative journalism being presented so that the news I read will present thorough and well-researched information about the topic at hand. This is not the case with this article.
Plumer began his piece by paraphrasing the Nuclear Regulatory Commission’s proposal on July 1 to overhaul its safety rules for radiation exposure at nuclear power plants. As he put it, the commission was concerned by the cost of the regulations and their tendency to “go beyond what is needed to protect human health.”
The NRC’s proposal asserted that current regulations often incur additional costs “without a measurable safety benefit”—for example, Plumer supplied, when regulators install additional equipment at plants in order to push radiation exposure “far below the legal limits.” Maximum dose limits, the agency said, are already set “well below levels associated with known health effects.”
This was meant to corroborate Plumer’s characterization about costliness, but Meyer noted the lack of substantiation:
You provide no rationale, evidence or citations for these claims, making simple conclusions about a very complex topic. How do you know that human health is indeed being protected, or as you imply, being over-protected? What examples can you provide of radiation exposure being “far below the legal limits”?
Trying to ‘simplify things’
Meyer focused on Plumer’s denial of “measurable safety benefits” from nuclear regulations, the premise of the central question Plumer posed in his piece: How much protection against low levels of radiation is worthwhile? Meyer took issue with Plumer’s framing:
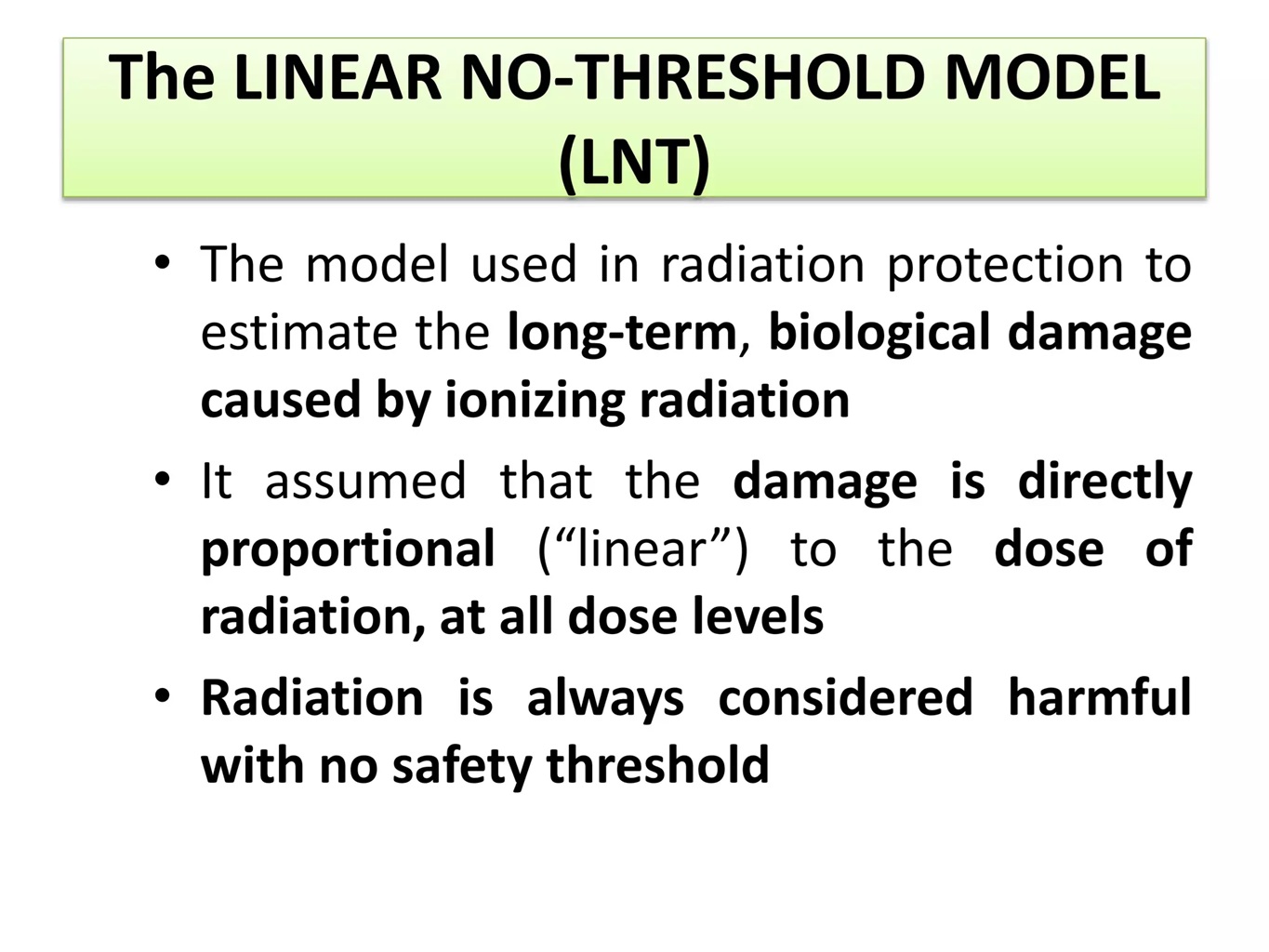
For decades, many researchers and regulators have tried to simplify things by adopting what’s known as the “linear no-threshold model,” which says that the effects of radiation scale down linearly with the dose, and that even tiny amounts of radiation can have small negative effects.
Calling the Linear No Threshold (LNT) model an attempt to “simplify things,” Meyer noted, is “a rather pejorative comment in light of the significant scientific evidence at hand”:
The 2006 National Academy of Sciences report on Biological Effects of Ionizing Radiation (BEIR VII) substantiates LNT, as did the 2021 NRC decision to deny a 2015 request to get rid of LNT.
Plumer “never mentions the history and current state of study and knowledge of the health effects of exposure to low levels of ionizing radiation,” Meyer said, pointing to 80 years of research:
The atomic photographer Robert Del Tredici includes a lengthy endnote in his 1985 book At Work in the Field of the Bomb, which recounts Karl Z. Morgan, the father of health physics—aka the study of the health effects of radiation—discussing how the effects of low-level radiation were well-researched in the late 1940s and were found to be significant. As Morgan’s medical perspectives raised public health questions about further expansion of the nuclear enterprise, they were minimized and ignored.
One of Plumer’s unquestioned and unexplored assertions especially stood out:
Experts agree that high doses of radiation are dangerous and can cause various types of cancer. But there’s much more disagreement about the effects of lower doses of radiation, such as the amounts that workers at nuclear power plants might receive in the course of their jobs. Different studies have found that low doses can be harmful, neutral or even beneficial.
The idea that low doses of radiation may be “even beneficial” refers to “radiation hormesis”—a widely dismissed claim of some nuclear promoters that exposure to radiation exercises the immune system and thus is healthy.
‘History of atomic press censorship’
“This piece,” said Meyer,
serves to promote the current government policies to greatly expand nuclear activities—it is not investigative journalism that thoroughly considers the topics at hand to give the public the information necessary for informed decision-making.
Meyer added: “The New York Times has an uncomfortable history of atomic press censorship.” Meyer cited as “a prime example” William Laurence, who, he noted, helped craft the official military line on Hiroshima while still ostensibly a Times journalist. Laurence was a Times science writer who also worked for the Manhattan Project, for which he drafted press releases and other government statements.
Back at the Times after the war, for years Laurence glorified nuclear technology. As author Beverly Deepe Keever wrote in her book News Zero: The New York Times and the Bomb, Laurence “served as a scribe writing government propaganda” to obscure the deadly and harmful effects of radiation.
More recently, Matthew Wald, who spent 38 years at the Times with a beat including the nuclear industry, left the paper in 2014 and the following year joined the Nuclear Energy Institute, the nuclear industry’s Washington-based trade group, as a policy analyst and communications consultant.
“Is history repeating itself, or can the New York Times cover the whole story here?” Meyer wrote. “The future of our genome is at stake.”
Meyer signed his letter as the treasurer of Physicians for Social Responsibility New York. He was also formerly the chapter’s president, the executive director of PSR Wisconsin, a longtime member of PSR’s national board, and the program director of the Alliance for Nuclear Accountability. He has not yet received a response from Plumer.
ACTION ALERT: You can send a message to the New York Times at letters@nytimes.com or via Bluesky: @NYTimes.com. Please remember that respectful communication is the most effective. Feel free to leave a copy of your message in the comments thread here.
Research Assistance: Emily Marie Spencer
Radiation Protection -analysis of NRC proposals
the US NRC is under pressure to weaken its current standards at a time when the scientific
evidence suggests these need to be tightened.
Tony Webb, July 2026.
Current standards under threat
Operating under a Directive from US President Donald Trump the US Nuclear Regulatory
Commission (NRC) proposes to weaken its current radiation protection standards – at a time when
the scientific evidence suggests these existing standards underestimate the risks faced by workers
and the public – and need to be significantly tightened. Unions, public health and environment
groups around the world are pressing governments, international and national protection agencies
to resist pressure from the USA to follow suit – and are calling for a comprehensive review the
evidence leading to increased worker and public protection.
In May 2025 US President Trump issued a Directive to the NRC to revise all its current regulations
and specifically those relating to radiation protection. It called for the NRC to abandon the
fundamental principle that underpins standards worldwide that there is no threshold or ‘safe’ level
of exposure to Ionising radiation. Any dose however small can be the one that triggers what are
known as ‘stochastic’ health effects that emerge over time from damage to individual cells in the
body – damage that is inadequately repaired and where the cells go on to reproduce in in
this damaged form, later manifesting as cancers, genetic, or other health damage. Some
other effects such as skin damage are called ‘deterministic’. A minimum or ‘threshold’ level
of exposure is required, and the severity of the damage increases with the level of exposure.
The severity of stochastic health effects is independent of the dose received – you either get
is or you don’t but the risk-probability that you do increases with the dose received over
your lifetime exposure.
Following from this principle that there is no safe level radiation standards required that all
exposures be kept ‘as low as reasonably achievable’ – known as the ALARA principle. . The
Presidential directive specifically instructed the NRC to reconsider this principle. It also required
review of the legal dose-limits for the amount of non-naturally occurring radiation that workers and
the public can be exposed to in any year. These annual dose limits have been set by national
standards agencies based mainly on international reviews of studies of Japanese survivors of the
bombing of the cities of Hiroshima and Nagasaki in 1945. These survivors who received relatively
large doses over a short time period. The level of damage to their health, notably their rates of
cancer has been tracked over time and used to estimate the probabilistic risk of stochastic damage
from lower doses spread over longer time periods using a ‘Linear No-Threshold’ (LNT) model –
essentially based on the no safe level principle. The risk estimates have been revised over time as
evidence emerged for higher cancer rates among the survivors and revision of the estimates of
doses they received that might have caused these cancers.
More recently large scale studies of nuclear plant workers in France the UK and USA – known as the
INWORKS studies (with more accurate measures of doses received and health effects compared to
non-exposed workers) have shown that the estimates used to set the current standards significantly
under-estimate the risk, and that the risk at low doses – over longer time periods may be
proportionately greater than the LNT model estimates suggest. These studies also show significantly
elevated levels or cardio-vascular diseases such as heart damage and strokes, and other worker
studies show elevated levels of dementia associated with radiation exposure. Together these
studies suggest there is an urgent need to comprehensively review the evidence of risks on which
the current national and international standards are based – particularly worker dose limits . In
addition recent meta analyses of cancer rates in large populations living close to nuclear power plants in Europe and the USA show that there is a significant general increase the closer people live
to these facilities particularly affecting the young and the elderly. These suggest the need to review
the standards that set dose-limits for public exposures alongside those reviewing expsore of
workers.
In short, the US NRC is under pressure to weaken its current standards at a time when the scientific
evidence suggests these need to be tightened.
The NRC proposals
Following the May 2025 Presidential Directive, the NRC has now, after several delays, released its
proposed revision of the standards. It clearly faced a dilemma as adopting the President’s suggested
changes would mean reversing its earlier 1991 decision that specifically rejected these same
proposals requested by industry lobbyists. In essence the 179-page proposal document (open for
45-days for comments) offers its reasoned judgements on the three key aspects of the review: the
LNT model, the ALARA principle and the occupational and public exposure limits.
To its credit the NRC retains the LNT as the basis for assessing risks at lower doses than those
received by Japanese bomb survivors. Hardly surprising as to have rejected this would have flown in
the face of international scientific pinion worldwide and its own 1991 decision. It does give some
credence the highly contested ‘Hormesis’ model based on limited studies suggesting that there may
be positive effects on health at low doses due to the capacity for cellular repair but ultimately
concludes that there is no scientific consensus that would support this or any other alternative to
the LNT model.
Unfortunately, proposes abandoning the ALARA principle arguing that it is subject to ‘excessive
subjectivity that leads to overly conservative assessments’ for managing exposures below the the
occupational and public dose limits. It is clearly identified as a burden on the nuclear industry – and
thus an impediment to the policy of reducing barriers to its development and operation. In its
place the NRC proposes ‘operating principles’ for managing doses below the legally enforceable
limits. Above (and perhaps only above) an expected dose of 100 mrem (1 MSv) per year – the limit
for public exposure – employees would need to be given ‘radiation worker training’. Above (and
again perhaps only above) an expected dose of 500 mrem (5 mSv) /year). i.e., at 10% of the
regulated exposure limit, employers would be required to monitor individual workers exposures. It
further suggests a cost-benefit approach for reducing exposures indicating that it would be
appropriate for employers to spend up to $5,200 (in 2014 US $) to avert each rem of occupational
exposure. If a radiation protection measure were more costly than that, the licensee would have an
acceptable cost-justified basis for not implementing the measure and instead accruing the dose as
long as that dose was within the regulatory dose limits.
The occupational dose limit is however further weakened by allowing exposures up to double the 5
rem (50 mSv) annual limit. Previously employers could apply for ‘planned special exposures’ for
situations needing higher worker-doses. These are no re-badged as ‘occupational dose limit
extensions’ (DLEs) permitting male workers (female workers are excluded) to receiving a dose of up
to 10 rem (100 mSV) in any year provided these do not result in the worker’s five-year average
exceeding the 5 rem (50mSv) annual limit – i.e. a total over any five year period of 25 rem (250 mSv).
These proposals will leave US workers facing permitted exposures greater than recommended by
international bodies and adopted by most national standards-setting agencies where the targeted
annual limit is 20mSv with exceptional exposures permitted up to 50 mSv provided these do not
exceed 20 mSv averaged over any five-year period. This 20 mSv annual averaging standard has been
in place since 1991 but was never adopted in the USA which retains the earlier 5 rem (50 mSv) annual limit. As indicated above the scientific evidence now calls for a revision of the stochastic
health damage risk estimates and a further tightening of the standards rather than their relaxation
as proposed by the NRC. Indeed it is notable that nowhere in the NRC proposals is here any mention
of, let alone critical review of the peer reviewed INWORKS studies.
The NRC does reject the Presidential Directive’s suggestion that the public exposure limit be raised
to 500 mrem (5 mSv). it leaves it at 100 mrem (1 mSv) in line with the international norm though it
does propose relaxing the emissions standards for radiation and radioactive material from nuclear
facilities from the existing 10 mrem to 25 mem. Again, these proposed relaxations come at a time
when the evidence suggests higher risks to the public living close to such plants and that a tightening
of existing standards is warranted. And again, nowhere does the NRC mention let alone critique this
evidence for increased health risks for populations living close to nuclear facilities.
International Opposition to the US NRC proposals
The NRC proposals are currently open for comments with a final decision on the revised regulations
due by the end of 2026. While any revised radiation protection standards will initially apply only to
the USA there are implications for radiation protection in other countries. Pressure on international
and national standards bodies can be expected. As well as the civil nuclear program it is expected
that the revised standards will apply to US based military facilities. Whether these US, or other
countries’ standards will apply to US military facilities and to any jointly owned civilian enterprises
based in other countries may be in doubt. In Australia for example a Naval Nuclear Powered
Submarine Safety Regulator (ANNPSR) has been created to oversee construction, operation,
maintenance, decommissioning and radioactive waste management from the UK, US (AUKUS)
nuclear submarine program. This new regulator reports to the Department of Defence and is
separate from the existing regulator, the Australian Radiation Protection and Nuclear Safety Agency
(ARPANSA) which reports to the Department of Health. How these regulators will collaborate, and
which standards will prevail is yet to be determined.
In Australia, as in other countries, notably the USA, Canada, coalitions bringing together the
concerns of trade unions, public health organisations and environment groups are campaigning for
rejection of the US NRC led proposals that would weaken current radiation protection standards
and for a comprehensive review of the scientific evidence that now strongly suggests the risks to
health of workers and the public are greater that when standards were last revised – now some 25
years ago – and need to be revised and significantly tightened.
Trump Administration Scrapping Nuclear Energy Rules Requiring Plants to Keep Radiation Levels “As Low as Reasonably Achievable”
Horrifying.
By Joe Wilkins, Jul 12, 2026, https://futurism.com/science-energy/trump-nuclear-regulation-radiation-energy
As government agencies go, the US Nuclear Regulatory Commission has left a lot to be desired, often operating less like a government watchdog and more as an industry partner. There’s fee recovery, for example, which effectively mandates the industry pay its own regulators’ salary, as well as the NRC’s habit of trusting voluntary leak reports from reactor operators, not to mention its history of hiding internal safety data to protect its reputation.
As if those deficiencies weren’t bad enough, president Donald Trump is now stripping what’s left of the commission’s mandate down to the bone. Last week, the NRC proposed a bold amendment to its long-standing nuclear safety principles: deleting a line requiring nuclear plant operators to keep radiation exposure “as low as is reasonably achievable.”
According to the Hill, the NRC justifies the move by saying it will remove “unnecessary ambiguity.” But critics say this rule is the whole reason energy companies bother keeping radiation levels as low as possible in the first place.
“Facility owners felt like… ALARA [as low as reasonably achievable] was forcing them to go well below the allowable radiation limits and spend a lot of money to do that,” director of nuclear power safety at the Union of Concerned Scientists Edwin Lyman told the Hill. “This is opening the door for sloppier practices,” Lyman continued, and “worse management.”
It gets worse. Also per the Hill, the NRC likewise announced plans to significantly weaken its approach to the National Environmental Policy Act, a foundational piece of legislation dating back to 1970. On Wednesday, the NRC said it wants to gut draft environmental reviews entirely — which, in practice, means kneecapping the public’s chance to weigh in before a reactor gets the green light.
If that weren’t enough, the commission also wants to wash its hands of its mandate to review basic environmental nuisances like noise, dust, and air pollution associated with nuclear facilities. That’s if they even do a review in the first place, as the proposed changes would exempt certain existing reactors, and even new reactors from regular inspection altogether, the Hill reports.
The proposed changes come just a few months after the US Department of Energy began stripping safety regulations that limited nuclear workers’ exposure to radiation. In effect, these changes allow energy companies to speed up productivity, unlocking higher profits at their workers’ expense.
The timing of it all is hard to overstate: with several new nuclear reactors gearing up for operations throughout the US, it’s clear the Trump administration is doing all it can to fast-track incoming nuclear facilities, consequences be damned.
Changes to radiation protection in the USA -could have been worse but are still bad.
Tony Webb 2 July 26
The US NRC has now released its proposed revisions to radiation protection standards
mandated by President Trump’s 2025 Directive (EO14300). It could have been worse. The
proposals do not completely abandon the established principle that there is no safe level of
exposure in favour of the contested view that low level exposures are ‘beneficial’. They do
not propose raising the existing permissible limits on exposure for workers and the public.
They do however abandon other important principles such as that all exposures should be
kept as low as reasonably achievable (ALARA) and give the nuclear industry flexible options
for a whole range of ‘operating procedures’ that can be used to control and limit exposures
– all overtly designed to ease the regulatory burden on the industry.
While repeatedly claiming that existing standards are already “conservative” these US
regulations already permit higher exposures than recommended internationally. The US 5
Rem (50 mSv ) occupational exposure limit is 2.5 times greater than the internationally
recommended limit used in most countries. Far from placing the proposals in the context of
the scientific evidence the proposals refer only to the outdated and flawed Life-span studies
of the Japanese bomb survivors who received high doses over short time periods rather
than studies of populations receiving low doses over longer time periods. In the whole 180-
page document outlining the proposed new regs I could not find a single mention of the
INWORKS studies of European and US nuclear plant workers that show the current
international standards underestimate the current internationally accepted level of
radiation-induced cancer risks used to set occupational exposure limits.
There is also no
mention of the increased risks for cardio-vascular diseases and dementia faced by such
workers and no mention of the studies of populations living close to nuclear plants that
show higher cancer rates – increasing the closer people live to these facilities. Buried in the
detail where devils usually hide there are also proposals that would weaken the so called
‘planned special exposures’ limits – the carve out that is used in the USA and elsewhere to
permit hiring of casual workers as ‘radiation sponges’ for the radiation-dirty jobs in annual
shutdown maintenance and clean-up operations for nuclear power plants. A closer reading
will probably reveal a more concerns but overall, the NRC proposals represent a significant
weakening of US standards that need to be opposed both within the USA and globally lest
they lead to weakening of standards or operating procedures for protection in other
countries. Other countries have reason to worry that joint operations with the USA (like the
Australian AUKUS nuclear submarine deal) and shared technologies that use these weaker
NRC standards as the basis for their design will be used as a backdoor for relaxation of
protection standards worldwide. US groups and others interested have 45 days to register
objections with the NRC to this latest Trump Dictated obscenity. Comments must be
submitted electronically using https://www.regulations.gov
On the positive side the legitimate concerns raised by these US proposals provide unions,
public health and environment groups in all countries with a ‘calling card’ to raise the demand with our national protection agencies for improved regulations for occupational
and public exposures in line with the available scientific evidence that shows current
standards need to be significantly tightened.
US moves to eliminate longtime radiation safety principle for nuclear power
“the change could ultimately make it so that currently low doses of radiation that workers and the public are exposed to “could increase really all the way up to regulatory limits without any sanction from the NRC.”
by Rachel Frazin – 07/02/26, https://thehill.com/policy/energy-environment/5951671-nuclear-power-radiation-exposure-nrc/
The federal government is proposing to overhaul radiation safety regulations for nuclear power, including by eliminating a long-term principle for nuclear safety.
The Nuclear Regulatory Commission (NRC) this week proposed to get rid of the requirement for nuclear plants to ensure that radiation exposure is “as low as is reasonably achievable.”
Proponents of the change say just using radiation dose limits is less subjective than going by the “as low as is reasonably achievable” principle — and that it led to overly conservative protections that stifled the nuclear industry.
Supporters of the current language, however, say that having the “as low as reasonably achievable” principle, also known as ALARA, in place ensures that nuclear plants take all measures possible to reduce exposure for workers and the general public.
NRC Chair Ho Nieh said in a statement that the agency is “raising the standard for regulatory clarity, not lowering the standard for safety.”
“Our radiation dose limits remain unchanged — what we’re eliminating is unnecessary ambiguity,” he said.
But critics say that eliminating ALARA means getting rid of a key incentive for energy companies to keep radiation levels as low as possible — and could mean more cancer cases.
“Facility owners felt like … ALARA was forcing them to go well below the allowable radiation limits and spend a lot of money to do that,” said Edwin Lyman, director of nuclear power safety at the Union of Concerned Scientists.
Lyman warned that the change could ultimately make it so that currently low doses of radiation that workers and the public are exposed to “could increase really all the way up to regulatory limits without any sanction from the NRC.”
He said this could include by having employees work longer shifts and therefore getting more radiation exposure.
Overall, he said, “this is opening the door for sloppier practices” and “worse management.”
In addition to axing ALARA, the NRC is proposing other changes, including loosening emissions limits for radioactive material.
It said that under one of the rules it is proposing to change, current regulations would allow for an estimated four excess cases of fatal cancer for every 10,000 people exposed to the maximum allowable radiation for 70 years. It said that the change it is making would allow this number to go up to nine cases for every 10,000 people.
It also proposed increasing how much radiation caregivers for people who receive radiation treatment can be exposed to.
The agency said that all of the changes it is proposing would save the industry about $9.53 million per year.
The moves come as the Trump administration has been pushing for the U.S. to build more nuclear power. Last year, an executive order from President Trump set the goal of quadrupling the nation’s nuclear power capacity by 2050.
It also directed the NRC to reconsider its use of ALARA and to speed up approvals for nuclear reactor licenses.
While the NRC is technically an independent agency, it is made up of three Republicans and two Democrats.
Last year, the White House fired a Democrat from the commission, which at the time, had a 3-2 Democratic majority. On Monday, the Supreme Court ruled the White House can conduct such firings.
US looking at easing restrictions on radiation exposure at the nation’s nuclear power plants
“This will only increase the disease burden at a time when cancer rates are already rising among younger people,”
The proposal would eliminate a standard to keep radiation exposure ‘as low as reasonably achievable’
The Independent, Rachel Dobkin in New YorkThursday 02 July 2026
Federal regulators are looking at easing restrictions on radiation exposure at the nation’s nuclear power plants.
The Nuclear Regulatory Commission, an independent agency aimed at ensuring the safe use of radioactive materials, proposed Wednesday eliminating a standard to keep radiation exposure “as low as is reasonably achievable,” also called ALARA.
ALARA is based on the linear no-threshold model, which presumes that any dose of radiation carries a proportional risk of harm.
The commission said in a press release that the proposal would introduce changes, including a graded approach to radiation dose management “based on risk and operational circumstances” and expanding options for managing workplace radiation exposure.
The Independent has reached out to the Nuclear Regulatory Commission for comment.
The changes could save the nuclear industry about $9.53 million a year, according to documents from the Nuclear Regulatory Commission obtained by The Hill.
Edwin Lyman, a physicist and nuclear safety advocate at the Union of Concerned Scientists, told Reuters, “In eliminating its use of the ALARA principle, the agency’s sweeping new proposed rule would allow nuclear facility workers and the general public to be exposed to higher levels of cancer-causing radiation just to save the nuclear industry money.”
“This will only increase the disease burden at a time when cancer rates are already rising among younger people,” Lyman said.
The number of new cancer cases increased among people under age 50 from 2010 through 2019, according to researchers at the National Institutes of Health.
The Nuclear Regulatory Commission noted in documents that the proposal would address part of President Donald Trump’s executive order to reform the agency. https://www.the-independent.com/news/world/americas/us-politics/nuclear-plants-radiation-exposure-rules-b3007995.html
US nuclear power regulator proposes changing rule protecting people from radiation

in eliminating its use of the As Low as Reasonably Achievable (ALARA) principle, the agency’s sweeping new proposed rule would allow nuclear facility workers and the general public to be exposed to higher levels of cancer-causing radiation just to save the nuclear industry money
By Timothy Gardner, July 2, 2026, https://www.reuters.com/legal/government/us-nuclear-power-regulator-proposes-changing-rule-protecting-people-radiation-2026-07-01/
Summary
- Proposal would eliminate the ALARA radiation protection standard and set objective dose limits
- NRC to take public comments on radiation rule for 45 days
- NRC Chairman Ho Nieh said change could help speed development of new reactors
WASHINGTON, July 1 (Reuters) – The U.S. nuclear power regulator on Wednesday proposed changes to a rule protecting people from radiation, the latest proposal pushed by the Trump administration to change or soften rules to speed development and cut costs for new atomic reactors.
President Donald Trump signed executive orders in 2025 seeking to speed up permitting of reactors and to overhaul the Nuclear Regulatory Commission and directing the Energy and Defense departments to work together to build nuclear plants on federal lands. Trump wants to quadruple U.S. nuclear power capacity by 2050 to meet power demands that are rising due to data centers, electric vehicles and crypto-currencies.
The Nuclear Regulatory Commission proposal eliminates a radiation protection standard called As Low as Reasonably Achievable, or ALARA, with objective dose limits for radiation. “This rulemaking is raising the bar on clarity in our regulations,” Ho Nieh, the NRC chairman, told reporters. “It is not lowering the bar on our safety standards.”
The industry has long argued that ALARA is tied to a model known as Linear No-Threshold that holds that any dose of radiation, no matter how small, carries cancer risks and that complying with ALARA is costly, time consuming, and full of uncertainties.
The proposed changes include adopting a graded approach to radiation dose management based on risk and operational circumstances. It also allows nuclear power plant operators greater flexibility to use “modern methods for evaluating radiation doses to workers and the public.”
Nieh said he does not anticipate that current nuclear reactors will make major changes due to the changed rule if finalized. But he said it could help speed development of new reactors.
“Now they have a very clear picture of what the requirements for radiation protection are going to look like, that will inform how they build and design their reactor, in terms of the shielding and the materials that they’re using,” Nieh told reporters.
Edwin Lyman, a physicist and nuclear safety advocate at the Union of Concerned Scientists, said the NRC has correctly reaffirmed the scientific consensus that there is no safe level of radiation exposure and that the cancer risk is proportional to the dose.
“However, in eliminating its use of the ALARA principle, the agency’s sweeping new proposed rule would allow nuclear facility workers and the general public to be exposed to higher levels of cancer-causing radiation just to save the nuclear industry money.”Nieh said he does not anticipate that current nuclear reactors will make major changes due to the changed rule if finalized. But he said it could help speed development of new reactors.
“Now they have a very clear picture of what the requirements for radiation protection are going to look like, that will inform how they build and design their reactor, in terms of the shielding and the materials that they’re using,” Nieh told reporters.
Edwin Lyman, a physicist and nuclear safety advocate at the Union of Concerned Scientists, said the NRC has correctly reaffirmed the scientific consensus that there is no safe level of radiation exposure and that the cancer risk is proportional to the dose.
“However, in eliminating its use of the ALARA principle, the agency’s sweeping new proposed rule would allow nuclear facility workers and the general public to be exposed to higher levels of cancer-causing radiation just to save the nuclear industry money.”
“This will only increase the disease burden at a time when cancer rates are already rising among younger people,” Lyman said.
Last month, the NRC proposed rule changes including changing a rule on security standards at nuclear power plants that UCS said would “dramatically weaken measures that protect their facilities from terrorist attacks.” Another rule proposed on Wednesday would make sweeping changes to reactor licensing including streamlining the construction of new reactors.
The NRC will take public comments on the radiation rule for 45 days before the rule is finalized.
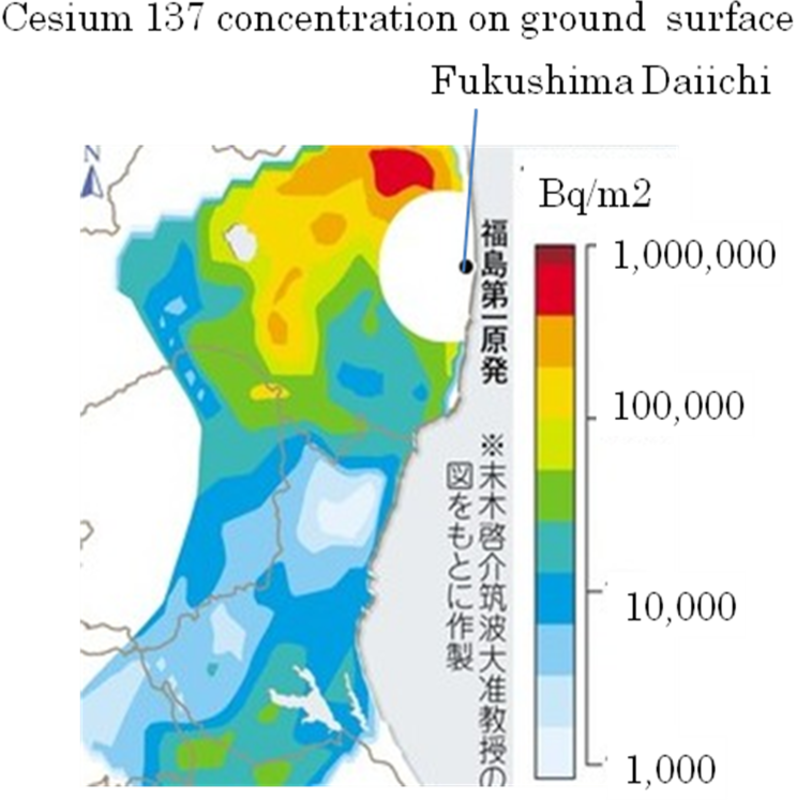
Radioactive cesium from 2011 Fukushima nuclear disaster spread over wide area: study
June 26, 2026 (Mainichi Japan), https://mainichi.jp/english/articles/20260626/p2a/00m/0na/004000c
TOKYO — A research team including members of the University of Tsukuba and National Taiwan University has clarified the dispersal routes of highly radioactive “cesium-rich microparticles” (CsMPs) released in the Fukushima nuclear disaster.
In the accident at Tokyo Electric Power Company Holdings Inc. (TEPCO)’s Fukushima Daiichi Nuclear Power Station in 2011, radioactive materials mainly contaminated areas to the plant’s northwest, but CsMPs were carried across a wide area of Fukushima Prefecture. The team also found that they were generated in large quantities four days after the March 11 Great East Japan Earthquake that year.
Actual extent of dispersal had remained unclear
CsMPs are spherical microparticles several micrometers in diameter. In the Fukushima Daiichi accident, they were formed when high-temperature nuclear fuel melted through to the floor and components of the melted concrete turned glasslike, encasing radioactive materials. The microparticles do not dissolve easily in water, and there are concerns that if inhaled they can remain lodged in the lungs, but the reality of how they spread had not been well understood.
The research team developed a method to examine the number of CsMPs contained in soil and analyzed soil samples taken from 100 locations in Fukushima Prefecture immediately after the accident. As a result, large numbers of CsMPs were found to the northwest and southwest of the plant, with as many as 52 particles per gram of soil. At some locations, 60% of the radioactivity in the soil was due to CsMPs.
The team then examined the dispersal process together with simulations of radioactive plumes, or air flows, and found that large-scale releases had begun in the early hours of March 15, 2011. A radioactive plume containing as many as 4,700 CsMPs per cubic meter was carried clockwise over a wide area of the prefecture, starting at the plant and moving from south to southwest and then northwest. It also reached Tokyo, the team said.
On the other hand, radioactive plumes released from 12 a.m. on March 16 onward contained no CsMPs. Instead, they are believed to have contained cesium in a form that easily dissolves in water.
‘Highly significant’ for future responses
Satoshi Utsunomiya, a National Taiwan University professor of environmental science on the team, said, “It is highly significant that we have clarified the process of when CsMPs were generated inside the plant and when their formation ceased.” The findings are expected to lead to decontamination efforts that better reflect actual conditions and to guidelines for responding to nuclear disasters.
Shinya Yamasaki, an associate professor of analytical chemistry at the University of Tsukuba, commented, “It has been shown that radiation maps and the distribution of CsMPs are different.”
The findings were published in the Journal of Hazardous Materials.
(Japanese original by Yurika Tarumi, Lifestyle, Science & Environment News Department)
NUCLEAR HOTSEAT. Women, Children At Greatest Risk from Nuclear Radiation – UN Report by Mary Olson, Dr. Amanda M. Nichols
This Week’s SPECIAL Featured Interview:
United Nations report on the generational impact of nuclear radiation on women and children, written by Mary Olson of Generational Radiation Impact Project and Dr. Amanda M. Nichols.
We all accept as proven scientific and medical fact that human exposure to ionizing radiation from nuclear weapons and their production is damaging to human health. But how do we know that? Who figures out how bad it can be? How much radiation we can be exposed to without risking our health? And how valid are those measurements?
We learn the alarming truth behind how those numbers were generated and what needs to be done instead from today’s guests, co-authors of the new report for the United Nations Institute for Disarmament Research, Gender and Ionizing Radiation: Towards a New Research Agenda Addressing Disproportionate Harm:
Mary Olson holds a degree in Evolutionary Biology and has been an educator on radiation health impacts while serving nuclear-impacted communities… and so much more. Her website is RadiationProject.org- Amanda M. Nichols, PhD, is a Postdoctoral Researcher in the Environmental Studies Program at the University of California, Santa Barbara. Nichols research focuses on illuminating the role of women in the North American anti-nuclear movement. Email contact: Dr.Amanda.M.Nichols@gmail.com
Gender and Ionizing Radiation: Towards a New Research Agenda Addressing Disproportionate Harm is cornerstone information in the movement to rid our planet of nukes. It is available for free downloa or pdf HERE.
Further References mentioned in the interview and additional Resources:……………………………………………………………
The Trump administration’s reckless attack on radiation protection will have long-term consequences for public safety

In the absence of an objective ALARA (as low as reasonably achievable) cost-benefit analysis, future decisions on limiting doses from ionizing radiation to workers and the public from nuclear power operations will be determined in significant part by the relative political strengths of industry and regulators. Under the Trump administration, the industry clearly has the upper hand.
Just as it did with air pollution rules, the Trump administration has now, in effect, set the value of American lives to zero in regulatory protections against nuclear-radiation-caused cancer.
the attacks of the Trump administration on public safety must be exposed.
By Frank von Hippel | Analysis | May 27, 2026, https://thebulletin.org/2026/05/the-trump-administrations-reckless-attack-on-radiation-protection-will-have-long-term-consequences-for-public-safety/?utm_source=ActiveCampaign&utm_medium=email&utm_content=The%20Trump%20admin%20s%20attack%20on%20radiation%20protection&utm_campaign=20260528%20Thursday%20Newsletter
Worldwide, regulations limiting doses from the radiation emitted by nuclear fissions and decays are based on the Linear No-Threshold (LNT) model. This hypothesis posits that, irrespective of whether ionizing radiation comes in a pulse or over years, the additional risk of developing cancer as a result is proportional to the cumulative amount of energy deposited per gram of tissue, with weighting risk factors for radiation type, sex, age, and specific organs.
Since 1975, the US nuclear industry has been required to limit exposures to workers and the public to “as low as reasonably achievable” (ALARA) levels. What the ALARA level should be is determined by cost-benefit analysis in which the costs of dose reductions are compared with the benefits to workers and the public, measured in terms of reduced disease and longer life expectancy.
In May 2025, four months after taking office, the Trump administration challenged this five-decade-old regulatory approach as part of an Executive Order “Ordering the Reform of the Nuclear Regulatory Commission” (NRC). The order claimed the “NRC utilizes safety models that posit there is no safe threshold of radiation exposure and that harm is directly proportional to the amount of exposure,” which corresponds to the linear hypothesis. “Those models lack sound scientific basis,” the Executive Order added, before directing the NRC to “reconsider reliance on the linear no-threshold (LNT) model for radiation exposure and the ‘as low as reasonably achievable’ [ALARA] standard, which is predicated on LNT.”
The Nuclear Regulatory Commission had reviewed exactly this question in 2021 in response to a campaign by advocates of the radiation “hormesis” theory, which posits that low doses of ionizing radiation actually protect against cancer by stimulating the body’s DNA repair mechanism—the exact opposite of ALARA. The NRC rejected that contention, concluding that “the LNT model continues to provide a sound regulatory basis for minimizing the risk of unnecessary radiation exposure to both members of the public and radiation workers.” As a result, the commission maintained the current dose limit requirements contained in its regulations.
But President Donald Trump’s decision to bring independent regulatory agencies under White House control and to fire the NRC’s chairman ended the commission’s resistance. On July 2, 2025, an anonymous NRC spokesperson enthused in a social media post that the Executive Order reforming the NRC “gives us a chance to reconsider our radiation protection framework in support of the whole-of-government effort to safely enable the nation’s use of nuclear power.”
Two weeks later, the NRC hosted a webinar for input on the issue of the LNT hypothesis. The Nuclear Energy Institute—the US nuclear industry’s lobbying organization—recommended that the commission remove ALARA and dose minimization as regulatory requirements. Instead, the institute proposed to establish a “practical threshold”—for instance, 2 rem per year (or 20 milliGray per year for gamma rays) for workers—below which further dose reduction would not be required. (The rem is a unit of effective absorbed radiation in human tissue, equivalent to one roentgen of X-rays. One millirem is one-thousandth of a rem. The Gray measures the absorbed dose, which is the physical amount of radiation energy absorbed by any material or tissue. One Gray corresponds to one Joule per kilogram.)
Radiation hormesis.
Read more: The Trump administration’s reckless attack on radiation protection will have long-term consequences for public safetyAdvocates of the theory of radiation “hormesis” do not believe the LNT hypothesis. Radiation hormesis is a fringe theory with passionate adherents who are taking advantage of the Trump administration’s skepticism about regulations of all types.
One of the most vocal hormesis advocates is Edward Calabrese, an emeritus professor of toxicology at the University of Massachusetts in Amherst. He argues that the evidence for the linear no-threshold hypothesis is based on scientific fraud and, therefore, should be replaced with a model that considers the possibility of no risk—and even possible benefits—from ionizing radiation below a certain dose.
Calabrese’s arguments persuaded some recent leaders of the Health Physics Society (HPS), an association of radiation-protection professionals, to host a 22-part, 10-hour video lecture series by Calabrese on the history of the LNT model in 2021-22. John Cardarelli, the HPS president when the videos were produced, summarizes Calabrese’s argument at the end of each video. In the final one, Cardarelli declares his conclusion that the LNT model is “based on flawed research, ideological motives, deliberate misrepresentation of the research record, and political agendas.”
Although the Health Physics Society declares that “the views expressed in these videos are not intended to represent official positions,” it also advertises that its associated credentialing organization, the American Academy of Health Physics, has “preapproved 10 continuing education credits for certified health physicists watching all 22 episodes of this video series.”
Physicist-epidemiologist Jan Beyea published a critique of Calabrese’s allegations in the HPS journal Health Physics, to which both Calabrese and Cardarelli have responded with lengthy rebuttals.
The research and reports Calabrese and his supporters are trying to discredit were done more than 50 years ago. For decades, the largest human population studied for radiation effects was the survivors of the 1945 Hiroshima and Nagasaki bombings, who, depending on their proximity to the ground zeros, were exposed to whole-body doses ranging from near zero to several Gray delivered in a single burst. But the cancer statistics for the Japanese survivors were not good enough to determine with high confidence carcinogenic effects in the dose range relevant for worker radiation protection (in the tens of milliGray per year). Hormesis advocates also argue that cellular mechanisms should be more effective in repairing the damage from low-rate radiation than from a nuclear explosion’s short pulse.
The lack of data on the effect of small low-rate doses left a gap in the epidemiological confirmation of the applicability of LNT estimates of the cancer risks from low doses to radiation workers and to civilian populations exposed to radioactive releases from nuclear accidents. That gap has been partially filled, however, in more recent studies of large populations of individuals who have received low-rate doses of ionizing radiation.
A directly relevant example is the INWORKS study done by an international consortium of researchers on the excess cancer deaths among approximately 310,000 nuclear industry workers in the United States, the United Kingdom, and France, whose radiation doses were measured and recorded throughout their decades of employment. As of 2012-16, this population had an average age of about 65, and about one third had died, with 28 percent of the deaths being due to “solid” cancers (abnormal masses of tissue arising in organs, glands, or bones), therefore excluding leukemia. Of those deaths, 5,500 to 14,000 were excess cases relative to the rate observed in a control group of 51,000 nuclear workers with near-zero occupational doses.
Figure 1 [on original]shows the rate of excess deaths from solid cancers in this population as a function of cumulative on-the-job dose 10 years before death, assuming that any solid cancer caused within the last decade of life would not have had time to become lethal. The bars show the 90-percent probability range associated with the number of deaths in each dose bin; that is, there is statistically only a 10-percent probability that, with more data, the number of excess deaths would converge outside that range (5 percent chance above and 5 percent below). The solid line is the best linear fit of the data to the LNT model.
By this measure, there are significant excess cancer deaths among nuclear workers down to cumulative doses of 30 milliGray.
Energy Department’s takeover. In addition to bringing the NRC to heel, the Energy Department’s Office of Nuclear Energy has been inviting startups promoting new-design nuclear power reactors to build prototypes on department land, including the 900-square-mile footprint of the Idaho National Laboratory, where they will not be subject to NRC safety requirements.
According to President Trump’s May 23 Executive Order, the NRC will be required “to approve reactor designs that the Defense Department or the Energy Department have tested and that have demonstrated the ability to function safely.”
At most, the startups will only be able to demonstrate that they will not have had a serious accident or a near miss within their first few years of operation before they hope to build their reactors in large numbers across the country and export them abroad. In their efforts to compete with natural gas, photovoltaic, and wind power plants, the nuclear startups are under great economic pressure to cut safety and security requirements currently required by the NRC and other regulators around the world. Costly requirements include containment buildings that prevent the release of radioactivity to the atmosphere in case of a core meltdown accident. Regulations also include requirements that it be possible for the timely evacuation of areas around the reactors where the population could be at risk of high radiation doses from an accident, and robust around-the-clock guard forces to protect nuclear plants against potential sabotage.
By putting the Energy Department, which is pouring billions of dollars into nuclear startups, first in line in safety regulation, the Trump administration has partially undone the 1974 decision of the post-Watergate Congress to separate safety regulation from nuclear power promotion by breaking up the Atomic Energy Commission to create the NRC and Energy Department.
Even before the Trump administration, under political pressure from the nuclear industry through congressional Republicans, the NRC commissioners backed off by majority vote from requiring filtered vents for a set of US reactors designed by General Electric that were clones of the Fukushima-Daiichi reactors 1–3, whose small-volume containments released large amounts of radioactivity due to overpressure after core meltdowns. The NRC also refused to end the practice of dense-packing spent fuel pools to five times their design density despite Fukushima unit 4’s near miss of a potentially much more catastrophic spent-fuel fire because of an undetected water level drop.
The end of ALARA. After it was effectively given much of the responsibility of regulating the US nuclear industry, the Energy Department commissioned a review of the LNT hypothesis by the Idaho National Laboratory, which supports the Office of Nuclear Energy’s mission to promote new types of nuclear power reactors.
INL quickly produced a report, which cited a 2013 comparison by Mohan Doss of the LNT model against the radiation hormesis, as “[p]erhaps most significant for regulatory considerations.” Dr. Doss is a radiologist, not an epidemiologist. His article was published in the journal Dose-Reponse, which was founded in 2003 with Professor Calabrese as its editor-in-chief and focuses on hormesis advocacy. Contrary to what the INL report claims, Dr. Doss’ article is not a meta-analysis but rather an argument for radiation hormesis.
Doss starts by arguing at length that the atomic bomb survivors study would have shown a hormesis effect had it been compared with a control group that had a higher incidence of cancer. Doss even replotted the atomic bomb survivor data to show the result if such a control group were used. In fact, there are appropriate zero-dose control groups for the atomic bomb survivors study, including those who were away from the cities at the time of the bombings. When those control groups have been used in studies, they showed some non-linearity with dose for male cancers, but no hormesis effect.
At the same time, INL referenced but ignored the findings of two actual meta-analyses of low-dose studies: one by the National Council on Radiation Protection and Measurements and one by an international team of 16 cancer epidemiologists led by Michael Hauptmann and published in the Journal of the National Cancer Institute and partly funded by the National Cancer Institute, National Institutes of Health, and the Energy Department.
The National Council review concluded that “no alternative dose-response relationship appears more pragmatic or prudent for radiation protection purposes than the LNT model.” Hauptmann and colleagues found that “there is evidence of cancer risks from low-dose ionizing radiation.”
INL’s “reevaluation report” was quickly cited in a memorandum by the Department’s Undersecretaries of Science and Nuclear Security recommending that the Secretary of Energy “eliminate ALARA from all Department of Energy Directives and Regulations,” which he reportedly has done.
In the absence of an objective ALARA cost-benefit analysis, future decisions on limiting doses from ionizing radiation to workers and the public from nuclear power operations will be determined in significant part by the relative political strengths of industry and regulators. Under the Trump administration, the industry clearly has the upper hand.
The Trump administration’s Environmental Protection Agency has recently made a similar decision that it will no longer take into account the health benefits from limiting air pollution. In 2024, the Biden administration announced new limits on fine particulate pollution from coal power plants and other facilities. Those regulations were justified by an estimate that, on average, 77 dollars in health benefits would result from each dollar spent by industry on emission reductions and that the regulations would save 4,500 lives per year.
A climate reporter commented in the New York Times about the Trump administration’s decision to roll back the air-pollution regulation that, for over four decades, “different administrations have used different estimates of the monetary value of a human life in cost-benefit analyses. But until now, no administration has counted it as zero.”
Just as it did with air pollution rules, the Trump administration has now, in effect, set the value of American lives to zero in regulatory protections against nuclear-radiation-caused cancer.
The damage that will result from the evisceration of the Nuclear Regulatory Commission will not be immediate and may arguably turn out to be minor on the scale of the damage the Trump administration is doing in other policy areas. But public safety analysts and decision makers must keep track of the dismantlement of regulatory structures that have been built over generations. Hopefully, it will be possible to reconstruct some of them, with improvements where possible. In the meantime, however, the attacks of the Trump administration on public safety must be exposed.
Nuclear test veterans hope for justice as secret files are released
Servicemen exposed to radioactive fallout in cold war weapons testing are using newly declassified documents to fight for a fair compensation scheme
In November 1957, thousands of servicemen on Christmas Island in the South
Pacific watched the testing of Britain’s first megaton thermonuclear bomb.
Witnesses compared it to seeing the end of the world.
Many viewed the
explosion on the island while wearing shorts and short-sleeved shirts, with
sunglasses handed out to protect their eyes. Veterans claim they were
exposed to needless risk and were the victims of gross negligence. Large
numbers later suffered blood disorders and cancers, which they believed
were caused by exposure to radioactive fallout. Most were denied war
pensions because of ill-health.
By contrast, those involved in the US
nuclear testing programme, including the Manhattan Project led by J Robert
Oppenheimer, benefited from a $2.6bn no-fault compensation fund. France
agreed in 2008 that it would pay compensation to nuclear test veterans who
suffered illness linked to radiation exposure.
British veterans now hope
the release of thousands of previously classified documents from the Merlin
files into the National Archives will help support their near-70-year
battle for justice. Some of these newly released documents analysed by The
Observer detail risks of radioactive fallout, health monitoring of military
personnel and orders for blood samples to be taken from servicemen that
could be used for evidence in any subsequent claims for damages.
Observer 24th May 2026, https://observer.co.uk/news/national/article/nuclear-test-veterans-hope-for-justice-as-secret-files-are-released
Newly Released Tritium Review Analyzes LANL Tritium Reports, Highlights Infant Doses
A newly released independent review of Los Alamos National Laboratory’s 2025 tritium venting raises serious concerns about radiation risks to children and infants and highlights major gaps in LANL’s public reporting and decision-making process.
The review also questions LANL’s decision to proceed with venting despite no measurable pressure buildup in the waste containers — meaning the explosion risk used to justify the releases may not have existed. https://www.ccwnewmexico.org/tritium
On May 14th, 2026, the Communities for Clean Water published the review analyzing two reports LANL released following its controversial September 2025 tritium release operations.
Authored by Dr. Arjun Makhijani, President of the Institute for Energy and Environmental Research (https://ieer.org/), the “Review of Los Alamos National Laboratory’s tritium venting reports – Volume 1 and Volume 2” provides a summary of the tritium venting as well as the data and estimates detailed in the two LANL reports.
1. FTWC Radioactive Air Emissions Summary, Volume 1: Stack Emissions & Off-Site Dose Consequence, LA-UR: 25-31093, November 14, 2025; and
2. FTWC Radioactive Air Emissions Summary, Volume 2: Environmental Sampling & Expanded Plume Modeling, LA-UR: 26-20967, February 17, 2026.
Notably, LANL formally acknowledged for the first time that estimated radiation doses to infants were more than three times higher than doses to adults — a change that came only after sustained public pressure and community participation in public meetings and hearings. Nevertheless, infant doses were not considered during the planning and modeling that took place prior to the tritium releases. LANL stated that infant doses would not be taken into account moving forward.
1 This Month
of the week – Hiroshima Nagasaki Day Coalition – Working together for the abolition of n\nuclear weapons – https://www.hiroshimadaycoalition.ca/


No Nuclear in Cwm Llynfi! Stop the nuclear power station near Maesteg.
To see nuclear-related stories in greater depth and intensity – go to https://nuclearinformation.wordpress.com
-
Archives
- August 2026 (102)
- July 2026 (355)
- June 2026 (287)
- May 2026 (306)
- April 2026 (356)
- March 2026 (251)
- February 2026 (267)
- January 2026 (308)
- December 2025 (358)
- November 2025 (359)
- October 2025 (375)
- September 2025 (257)
-
Categories
- 1
- 1 NUCLEAR ISSUES
- business and costs
- climate change
- culture and arts
- ENERGY
- environment
- health
- history
- indigenous issues
- Legal
- marketing of nuclear
- media
- opposition to nuclear
- PERSONAL STORIES
- politics
- politics international
- Religion and ethics
- safety
- secrets,lies and civil liberties
- spinbuster
- technology
- Uranium
- wastes
- weapons and war
- Women
- 2 WORLD
- ACTION
- AFRICA
- Atrocities
- AUSTRALIA
- Christina's notes
- Christina's themes
- culture and arts
- Events
- Fuk 2022
- Fuk 2023
- Fukushima 2017
- Fukushima 2018
- fukushima 2019
- Fukushima 2020
- Fukushima 2021
- general
- global warming
- Humour (God we need it)
- Nuclear
- RARE EARTHS
- Reference
- resources – print
- Resources -audiovicual
- Weekly Newsletter
- World
- World Nuclear
- YouTube
-
RSS
Entries RSS
Comments RSS
