Asking the tough questions on Fukushima
What a load of spun crap, to be polite: “Moreover, the government is lifting the evacuation order for any areas where annual radiation levels are “no more than” 20 mSv. The International Commission on Radiological Protection told the government that once the situation had stabilized in the affected areas, people could return if radiation dropped to between 1 and 20 mSv, but the lower the better. Exposure to 20 mSv for a short period may not be a problem, but it could have harmful effects in the long run.”

In the thick of it: Industry Minister Yosuke Takagi (right) is exploring a variety of options to boost agricultural areas near the crippled Fukushima No.1 nuclear power plant.
In January, regional newspaper Fukushima Minpo interviewed Yosuke Takagi, state minister of economy, trade and industry. While talking about reconstruction plans for areas near the crippled Fukushima No. 1 nuclear power plant, Takagi mentioned resurrecting Dash-mura (Dash Village), a farm created from scratch by boy band Tokio for its Nippon TV series “The Tetsuwan Dash.”
The location of Dash-mura was always secret, lest Tokio’s fans descend on the project and destroy its rustic purity. But following the reactor accident caused by the Great East Japan Earthquake, it was revealed that the farm was in an area declared off-limits due to its proximity to the plant. It was promptly abandoned.
A different news outlet, Fukushima Minyu, clarified that the revival of Dash-mura is “nothing more than a personal idea of Takagi’s,” but that he intends to discuss it with related parties. An 80-year-old farmer who once worked with Tokio on the project told Minyu that bringing back the farm would be a great PR boost for the area’s agriculture, which is obviously Takagi’s aim. The show’s producer, however, after hearing of Takagi’s comment, tweeted that he knew nothing about the news, adding cryptically that “Dash-mura is no one’s thing.”
The Huffington Post called the Ministry of Economy, Trade and Industry to ask if it had any intention of reviving Dash-mura. A representative only “confirmed” that Takagi had “made such a comment” and said METI had no “definite plan” to that end but might “study it.”
Nevertheless, the idea fits in with the government’s goal of getting former residents to move back to the area. Last week, authorities announced they would further reduce the evacuation zone at the end of the month, which means it will have shrunk by 70 percent since April 2014. The concern is that few people want to return. Some have already made lives for themselves elsewhere and see a lack of opportunity in their old communities.
Many also remain suspicious of the government’s assurances that radioactivity has dropped to a safe level. There is still debate among experts as to whether or not the radiation in the area is dangerous. The government says that the problems caused by the accident are now “under control,” and affected residents can soon go back to their old lives.
One media outlet who has challenged this assumption is TV Asahi’s “Hodo Station.” On March 9, the nightly news show sent its main announcer, Yuta Tomikawa, to Iitate, a village located about 40 km from the crippled nuclear facility. All 6,000 residents were eventually evacuated after the accident.
Standing in front of rows of black plastic bags, Tomikawa reported that, according to the government, decontamination efforts have been a success. A safe annual radiation level is 1 millisievert, but a local dairy farmer told Tomikawa that his own readings showed five times that level, adding that 70 percent of Iitate is wooded and forest land had not been decontaminated yet.
Moreover, the government is lifting the evacuation order for any areas where annual radiation levels are “no more than” 20 mSv. The International Commission on Radiological Protection told the government that once the situation had stabilized in the affected areas, people could return if radiation dropped to between 1 and 20 mSv, but the lower the better. Exposure to 20 mSv for a short period may not be a problem, but it could have harmful effects in the long run.
Tomikawa did not say that people who returned to Iitate would be in danger, but he did imply that the government is manipulating numbers in an attempt to persuade evacuees to return to their homes.
The web magazine Litera wrote that TV Asahi is the only mainstream media outlet to question the government line in this regard. Actually, Nippon TV did something similar, albeit indirectly. Last month, it rebroadcasted an episode of its “NNN Document” series about the married manzai (stand-up comedy) duo Oshidori Mako-Ken’s efforts to come to terms with the Fukushima meltdowns and their aftermath.
The couple belongs to the large Osaka-based entertainment company Yoshimoto Kogyo, but ever since the disaster Mako has attended about 500 related news conferences, making a nuisance of herself by plying Tokyo Electric Power Company Holdings employees and government officials with questions the mainstream media don’t usually ask.
In order to gain access to the news conferences, she offered stories to the weekly magazine Spa! Her editor there told Nippon TV that Mako is now respected or resented by a lot of full-time journalists, partly because she’s a geinojin (entertainer) who has proved her mettle as a reporter, but mainly because of her hard-line queries, which put her interlocutors on the spot.
Following the disaster, Mako became suspicious when she saw people fleeing Tokyo in large numbers but heard nothing about it on the news. In order to make sense of the situation she’d watch unfiltered news conferences about the disaster on the internet. She realized only independent reporters asked tough questions, so she started attending them herself as a proxy for average people who didn’t understand what was going on. The more officials obfuscated, the more she studied.
She’s now recognized by some foreign press as one of the most informed persons on the subject — she even received a letter of encouragement from Pope Francis — and yet she’s shunned by the Japanese press. Nevertheless, she has dedicated followers, including workers cleaning up the reactor who often feed her questions to ask of officials. She’s won awards for her work, but from citizens groups, not media groups.
Nowadays, Mako and Ken do more free lectures on Fukushima No. 1 than they do comedy shows. One of their main themes is that media reports tend to confuse the public rather than inform them, but that’s really the fault of the government, which would like nothing better than for people to feel as if nothing ever happened.
Press conference at FCCJ on The Dangers of Low-Dose Radiation in Fukushima
Six years after the Fukushima nuclear accident, concerns about low-dose radiation and the decision to reopen much of the evacuation zone to returning evacuees have not been settled. Representatives from the Citizen-Scientist International Symposium on Radiation Protection (CSRP), a non-profit organization based in Tokyo, will explain their concerns and outline their recommendations, which have been signed by experts belonging to scientific organizations from all over the world.
The recommendations are addressed to Japanese authorities in charge of risk communication and radiation protection measures in the area affected by radiation from the Fukushima Daiichi Nuclear Power Plant.
The scientists take a critical look at risk communication currently conducted by the Japanese authorities and list urgent action that is required on behalf of the victims of the nuclear accident. They recommend using the “linear non-threshold model” based on the latest scientific findings and challenge the present return policy for the evacuees to areas below 20 mSv of radiation.
These recommendations are published in the science journal Kagaku in March 2017 and they will also be presented to Japan’s environment minister, the director general of the Reconstruction Agency and the governor of Fukushima Prefecture.
No Return to Normal in Fukushima
Just 6 years ago Fukushima was struck by a deadly earthquake, and then a nuclear disaster. For the survivors, there’s been no return to normal.
After Fukushima disaster, Japanese mothers don lab coats to measure radiation

IWAKI, Japan, March 9 (Thomson Reuters Foundation) – At a laboratory an hour’s drive from Japan’s Fukushima nuclear plant, a woman with a white mask over her mouth presses bright red strawberries into a pot, ready to be measured for radiation contamination.
Six years after a massive earthquake off the coast of Japan triggered meltdowns at three of Fukushima’s reactors, local mothers with no scientific background staff a laboratory that keeps track of radiation levels in food, water and soil.
As some women divide the samples between different bowls and handmade paper containers, others are logging onto computers to keep an eye on data – findings that will be published for the public to access.
The women on duty, wearing pastel-coloured overalls, are paid a small salary to come in for a few hours each day, leaving them free to care for their children after school.
“In universities, data is handled by qualified students, who have taken exams qualifying them to measure radiation. Here, it’s done by mothers working part-time. It’s a crazy situation,” laughed Kaori Suzuki, director of Tarachine, the non-profit organisation that houses the mothers’ radiation lab.
“If a university professor saw this I think they would be completely shocked by what they see.”
Tarachine was set up 60 km (40 miles) down the coast from the Fukushima plant, in the city of Iwaki. After the magnitude 9 quake struck on March 11, 2011, triggering a tsunami, authorities declared a no-go zone around the plant.
Iwaki lay outside its 30 km radius, with lower radiation levels compared to the rest of Fukushima prefecture.
But with public announcements advising locals to stay indoors in the aftermath of the worst nuclear calamity since Chernobyl, the “invisible enemy” of radiation has continued to worry the mothers working at the lab.
“As ordinary citizens we had no knowledge about radiation at all. All we knew was that it is frightening,” said Suzuki.
“We can’t see, smell or feel radiation levels. Given this invisibility, it was extremely difficult for us. How do we fight it? The only way is to measure it.”
To supplement readings by the Japanese government and the Tokyo Electric Power Company (TEPCO) that manages the nuclear plant, Tarachine publishes its own findings every month.
With donations from the public that helped them buy equipment designed to measure food contamination, the mothers measure radioactive isotopes caesium 134 and 137, and collect data on gamma radiation, strontium 90 and tritium, all of which were released during the Fukushima disaster.
Strontium-90 gravitates toward the bones when absorbed by breathing it, drinking it in water, or eating it in food. It can remain for years, potentially causing bone cancer or leukaemia.
Tritium goes directly into the soft tissues and organs of the human body. Although it is less harmful to humans who are exposed to small amounts of tritium every day, it could still be a hazard for children, scientists say.
The mothers say other parents trust the lab’s radioactivity readings in local food more than those from the government.
“This issue is part of everyday life for these mothers, so they have the capability to spot certain trends and various problems rather than just accumulating expert knowledge,” said Suzuki.
To handle potentially dangerous materials, the mothers have to study for exams related to radiation and organic chemistry.
“At the beginning I was just completely clueless. It gave me so much of a headache, it was a completely different world to me!” said Fumiko Funemoto, a mother of two, who measures strontium 90 at the lab.
“But you start to get the hang of it as you’re in this environment every day.”
As the lab only accepts items for testing from outside the exclusion zone, most results show comparatively low radiation levels.
But Suzuki says this is an important process and is especially reassuring to the parents of young children. The women also measure radiation levels in sand from the beach, which has been out of bounds to their children.
“If the base is zero becquerels (unit of radiation), and there is, say, 15 or 16 becquerels of caesium, that’s still higher than zero. That means there is slightly more risk,” Suzuki said.
“There are also times when you’re like, ‘Oh, I thought levels were going to be high there – but it’s actually ok’. The importance lies in knowing what’s accurate, whether it’s high or low … unless you know the levels, you can’t implement the appropriate measures.”
Since official screenings began following the nuclear accident, 174 children in Fukushima prefecture have been diagnosed with – or are suspected of having – thyroid cancer, according to figures from Fukushima’s local government.
Despite the International Atomic Energy Agency (IAEA)reporting in 2015 that an increase in thyroid cancer is unlikely, the mothers insist there is value in their work.
The first pictures from inside the nuclear plant were released by TEPCO in January, announcing it may have found nuclear fuel debris below the damaged No. 2 reactor – one of three affected by the 2011 disaster.
“In general, the issue of nuclear power is not really talked about much these days. It was talked about after the accident for about a year or so, but today, conversations mentioning words like ‘radiation’ don’t happen anymore,” Funemoto said.
“But I think the reality is different. The radiation isn’t going to go away. That’s why I’m doing this. So many places are still damaged. This idea that it’s safe and that we shouldn’t be anxious doesn’t really add up.”
Ai Kimura, another mother agrees. “My parents think I’m a bit paranoid. They keep saying, ‘it’s okay isn’t it?” she said.
“But what if there’s a chance that in 10 or 20 years time, my own child gets thyroid cancer? And I could have done my bit to minimise the risks. My children are mine and I want to do whatever I can to protect them.”
http://uk.reuters.com/article/japan-women-radiation-idUKL8N1G66K0
Die-offs on US West Coast linked to Fukushima radiation???

Charles Perrow, Yale University professor emeritus and Stanford University visiting professor, published Apr 2016 (emphasis added):
Could I just make an observation that’s been missing from this interesting discussion? Fukushima accident is not over – not by any means…
The cancer rate in Japan is going to rise steadily. It’s going to be denied by the government because there’s no transparency on this issue in Japan.
There’s a particular example of the problem that intrigues me is when they put the plant in, they not only dug it out so it’d be closer to the water source – the sea – but they put it where there was a river flowing underneath that area. They went up the hill and they diverted the river so that it flowed down on the sides of the large area there and that was no problem. They never anticipated an earthquake could wreck their diversion.
So know we have a strong underground river flowing directly under the plant where three huge globs of molten fuel are sitting on the bottom, giving off radiation, and sending that radiation into the water through the river that’s underneath the plant.
And it’s going out into the ocean and we’re seeing damage in the marine life on the West Coast of the U.S. and British Columbia.
There’s no way that’s going to be stopped until they get the molten cores out of there, and they have no way — that they know of — of doing that. Nobody has any idea what to do about the continuing Fukushima contamination.
Watch Perrow’s comments on Fukushima here (at 1:34:30 in)
Professor Sonja Schmid at 1:39:16
“The question of nuclear becomes a question of democracy and ultimately a question of justice. Who gets to say something? And whether we entrust these decisions to governments and technocrats, or how, if we decide to do so, we democratize the process. And it’s challenging no matter how you plan to go forward, but I think that’s the ultimate lesson of this, that we can no longer have technocrats, scientists and engineers in charge defining “the real risk” and then solving it, and the rest of the population just watches and has no impact whatsoever on these questions or how they are being addressed.”
Charles Perrow’s paper “Nuclear Denial”, published in the Bulletin of the Atomic Scientists in 2013
Sonja Schmid is a professor at Virgina Tech. From her bio: “Sonja Schmid teaches courses in social studies of technology, science and technology policy, socio-cultural studies of risk, energy policy, and nuclear nonproliferation. She is particularly interested in examining the interface of national energy policies, technological choices, and nonproliferation concerns. “
http://www.cornell.edu/video/five-years-after-fukushima-lessons-learned-nuclear-accidents
Ocean survey 1.5 km off the coast of Fukushima Daiichi
Results collected in an ocean survey 1.5 km off the coast of Fukushima:
Cesium 137 – 51.6 Bq/kg
Cesium 134 – 16.5 Bq/kg
Strontium 90 – 1.92 Bq/kg
Fukushima 6 Years After: No Return to Normal
The Japanese government is set to lift evacuation orders in heavily contaminated areas around Fukushima. It will cut compensation and housing support to survivors, who are still struggling six years later.
Their basic rights to health, housing, and environment are being violated. The government is desperately trying to minimize the disaster at the expense of survivors in an attempt to revive the dying nuclear industry and suffocate other cleaner energy sources. We must say no!
Greenpeace has just published report on the Fukushima disaster entitled “No return to normal”. They made a study of the potential doses of the inhabitants who would return to the evacuated areas, with a focus on Iitate-mura. http://www.greenpeace.org/japan/Global/japan/pdf/NRN_FINweb4.pdf
The report is based on many on-site measurements and makes lifetime dose assessments. It should be noted that the samples were taken by the citizen laboratory Chikurin, founded with the support of the ACRO. http://chikurin.org/
The authorities planned to lift the evacuation order at the end of March in Iitaté-mura, except in areas classified as difficult return zones, as well as in the Yamakiya district of Kawamata. Compensation will stop within one year. This concerns more than 6,000 people in Iitate who are facing a dilemma, as in all the other contaminated territories.
Greenpeace recalls that decontamination concerns only areas close to dwellings and cultivated fields and that forest covers 75% of this mountainous area. Even in areas where decontamination work has been carried out, the doses remain high. Greenpeace carried out measurements of soil contamination and dose in 7 dwellings to estimate the exposure for people who would return. This varies between 39 and 183 mSv over 70 years from March 2017. This may exceed the limit of 1 mSv / year which is the dose limit in normal time and the total dose of 100 mSv from which the Japanese authorities admit that there is an increased risk of cancer. The doses taken at the beginning of the disaster are not taken into account in this calculation.
In its calculations, the government estimates that the dose rate is reduced by 60% in homes due to the screening effect of the walls. But the measurements made by Greenpeace in a house show that the reduction in exposure is not as strong.
Source: http://fukushima.eu.org/fukushima-6-ans-apres-rapport-de-greenpeace/
Translation Hervé Courtois
‘The cancer rates have surged enormously due to high levels of radiation’
By Christopher Busby
The US Nuclear Regulatory Commission has killed a study aimed at finding out whether nuclear reactors pose cancer risks to nearby residents. According to the Los Angeles Daily News, the decision was made due to the high cost of the probe and doubts that it would prove effective. The project in question, which is worth eight million dollars, would have examined seven nuclear facilities all across the country. The new investigation was supposed to have reassured Americans that it was not dangerous healthwise to reside near a nuclear power plant. A similar study, coming to the same conclusion, was last conducted almost 30 years ago. Several recent European tests revealed rather disturbing links between cancer and minors living close to nuclear facilities. Radio Sputnik discussed the issue with Christopher Busby, British scientist known for his theories about the negative health effects of very low-dose ionising radiation. Mr. Busby is a director of Green Audit Limited and scientific advisor to the Low Level Radiation Campaign.
https://soundcloud.com/radiosputnik/the-cancer-rates-have-surged-enormously-due-to-high-levels-of-radiation-christopher-busby
‘Fukushima catastrophe ongoing: Leakage on a daily basis’

There are many shoes still to drop at Fukushima Daiichi, said Kevin Kamps, radioactive waste monitor at Beyond Nuclear. If something goes wrong with the radioactive waste storage pools, there could be a release of high-level radioactivity into the air, he added.
Radiation at Fukushima’s nuclear power plant is at its highest level since the tsunami-triggered meltdown nearly six years ago. Tokyo Electric Power Company (TEPCO) is reporting atmospheric readings inside Daiichi’s reactor No.2 are as high as 530 sieverts an hour, while a human exposed to a single dose of 10 sieverts would die in a couple of weeks.
RT: Can you explain what is likely going on here?
Kevin Kamps: This catastrophe that is ongoing is nearly six years old at this point. The fuel, the melted cores have been missing an action. TEPCO doesn’t know where they are; the Japanese government doesn’t know where they are; nobody knows where they are. What could have happened is these probes, these cameras, these robots, these radiation monitors that are being sent in by TEPCO to try to figure out what is going on, may have encountered the closest they have come yet to these melted cores. They may even have come upon melted fuel that is not under water, and water serves as a radiation shielding. So if this is an open area and there is no water – that could explain.
But what you’ve got are melted reactor cores. Of course, human beings can’t be in operating atomic reactors. They also can’t be in this area where there is a meltdown. There is also imagery – it looks like a melt through of a metal grade. It all stands to reason that the cores melted through the reactor pressure vessels and down into the containment structures right through that metal grating.
It is not unexpected, but we still don’t know where the cores are. There are claims that “it’s all contained, don’t worry about it.” It is indisputable that there is a daily flow of radioactively contaminated groundwater into the ocean. The figures something like 80,000 gallons per day of relatively low-level radioactive waste water. Then you’ve got those storage tanks – we’re talking 800,000 tons of highly radioactive water stored in tanks. Every day they pour a hundred tons of water on each of these three melted down cores. Sometimes they lose those tanks. They leak, they overflow – it is an ongoing catastrophe.
RT: So the contamination, in this case, could leak out, couldn’t it?
KK: There is some leakage on a daily basis. Then they try to capture as much as they can and contain it in the storage tanks, which they sometimes lose, whether during a typhoon or through human error – they have had overflows. So many shoes can still drop at Fukushima Daiichi. One of the ones is the high radioactive waste storage pools that aren’t even inside radiological containment. They don’t have all of that spent nuclear fuel transferred to a safer location in a couple of the units still. If something were to go wrong with that – those would be open air releases of very high-level radioactivity.
The prime minister at the time the catastrophe began, [Naoto] Kan, had a contingency plan to evacuate all of North-East Japan – up to 50 million people. It was predominantly because of those storage pools. We’re still in that predicament- if one of those pools were to go up in flames. As Tokyo plans to host the 2020 Olympics and bring in many millions of extra people into this already densely populated area -it is not a good idea.
RT: Going back to this specific leak: how does this complicate the cleanup efforts there? Is it possible even to get something in there right now to examine what is going on?
KK: State of the art robotic technology – Japan is a leader in robotics – can only last so long, because the electronics get fried by the gamma radiation, and probably neutron radiation that is in there. That is the situation deep in there. They are already saying it will take 40 years to so-called decommission this, but that may be optimistic.
RT: Also in December the government said it is going to take twice as much money – nearly twice as much as they originally thought – to decommission that. Does this make matters ever worse – this leak? Or is this just kind of the situation to expect at this point?
KK: It just shows how dire the situation is. The figures of $150 billion to decommission – I have seen figures from a think tank in Japan sided by Green Peace Japan up to $600 billion. If you do full cost accounting: where is this high-level radioactive waste going to go? It is going to need a deep geological depository. You have to build that and operate it. That costs a hundred billion or more. So when you do full cost accounting, this catastrophe could cost hundreds of billions of dollars to recover from. We’re just in the beginning.
https://www.rt.com/op-edge/376607-leakage-radiation-fukushima-japan/
Up to 4.20µSv near the Fukushima Tetsuzan water dam
This short article is dedicated to a pro-nuke troll, whose alias is Octo.
Octo, should I indulge the reader, is usually present at the chat of the “Fukushima Diary” blog. He enjoys pushing his propaganda of how nuke is safe.
How Tepco is doing a terrific job at Fukushima Daiichi and is in total safety control of everything.
How radiation is now very low in Fukushima How the fish and seafood is now safe etc.
Everyone is believing his crap *cough*, but he, like all of the other bewildered, confused and baffled Japanese *experts? never gives up.
Watching this video, I am thinking about him and his continuous lies, and also all those other Japanese pro-nuke trolls that I encountered on internet in the past few years.
This video was shot last November 2016 South of Soma, it is the mountain trail to reach the Tetsuzan dam, a place approximately 20km from the Fukushima Daiichi nuclear plant.

I think all those disinformation spinners paid by Tepco, Dentsu or Government, whose job is to spread lies about the Fukushima disaster on blogs, forums and Facebook, should all go living up there, as they claim it is now completely safe.
They should breath the good air from Fukushima, eat everyday very safe Fukushima rice and vegetables, and of course eat also plenty of safe fish and seafood, and drink plenty Fukushima safe water.
I would give them only one word of advice :
“Don’t forget to smile,
Smile a lot everywhere and everyday, so that the radiation won’t affect you.”
Special credit to the Fukuichi Citizen Radiation Monitoring Project
Radiation level at Fukushima reactor highest since 2011 disaster; grating hole found

TOKYO (Kyodo) — The radiation level inside the containment vessel of the No. 2 reactor at the crippled Fukushima Daiichi nuclear complex stood at 530 sieverts per hour at a maximum, the highest since the 2011 disaster, the plant operator said Thursday.
Tokyo Electric Power Company Holdings Inc. also announced that based on image analysis, a hole measuring 2 meters in diameter has been found on a metal grating beneath the pressure vessel inside the containment vessel and a portion of the grating was distorted.

According to TEPCO, the extremely high radiation level was found near the entrance area in the space just below the pressure vessel. The previously highest radiation level monitored in the interior of the reactor was 73 sieverts per hour.
The hole could have been caused by nuclear fuel that penetrated the reactor vessel as it overheated and melted due to the loss of reactor cooling functions in the days after a powerful earthquake and tsunami on March 11, 2011 hit northeastern Japan.
According to the image analysis, about 1 square meter of the grating was missing.
The plant operator plans to deploy a robot at the bottom of the reactor containment vessel, which houses the reactor pressure vessel, to check the conditions there.
The analysis follows TEPCO’s discovery Monday of a black mass deposited on the grating directly beneath the pressure vessel, possibly melted fuel after the unit suffered a meltdown along with two other Fukushima Daiichi reactors.
Images captured using a camera attached to a telescopic arm on Monday also showed part of the grating has gone. A further analysis of the images found a 2-meter hole in an area beyond the missing section on the structure.
If the deposits are confirmed as fuel debris, it would be the first time the utility has found any at the three units that suffered meltdowns.
Following one of the world’s worst nuclear disasters since the 1986 Chernobyl catastrophe, the No. 1 to 3 reactors suffered fuel meltdowns.
Portions of the fuel in the reactors are believed to have melted through the pressure vessels and accumulated at the bottom of the containment vessels.
The actual condition of the melted fuel has remained unknown due to high radiation levels.
http://mainichi.jp/english/articles/20170202/p2g/00m/0dm/087000c
http://mainichi.jp/articles/20170203/k00/00m/040/079000c

Genetic radiation risks: a neglected topic in the low dose debate.
Abstract
Objectives
To investigate the accuracy and scientific validity of the current very low risk factor for hereditary diseases in humans following exposures to ionizing radiation adopted by the United Nations Scientific Committee on the Effects of Atomic Radiation and the International Commission on Radiological Protection. The value is based on experiments on mice due to reportedly absent effects in the Japanese atomic bomb (Abomb) survivors.
Methods
To review the published evidence for heritable effects after ionising radiation exposures particularly, but not restricted to, populations exposed to contamination from the Chernobyl accident and from atmospheric nuclear test fallout. To make a compilation of findings about early deaths, congenital malformations, Down’s syndrome, cancer and other genetic effects observed in humans after the exposure of the parents. To also examine more closely the evidence from the Japanese A-bomb epidemiology and discuss its scientific validity.
Results
Nearly all types of hereditary defects were found at doses as low as one to 10 mSv. We discuss the clash between the current risk model and these observations on the basis of biological mechanism and assumptions about linear relationships between dose and effect in neonatal and foetal epidemiology. The evidence supports a dose response relationship which is non-linear and is either biphasic or supralinear (hogs-back) and largely either saturates or falls above 10 mSv.
Conclusions
We conclude that the current risk model for heritable effects of radiation is unsafe. The dose response relationship is non-linear with the greatest effects at the lowest doses. Using Chernobyl data we derive an excess relative risk for all malformations of 1.0 per 10 mSv cumulative dose. The safety of the Japanese A-bomb epidemiology is argued to be both scientifically and philosophically questionable owing to errors in the choice of control groups, omission of internal exposure effects and assumptions about linear dose response.
Keywords: Congenital malformation, Down´s syndrome, Environmental radioactivity, Internal radiation, Low level effects, Sex-ratio, Still birth
Introduction
The most serious effects of ionizing radiation–hereditary defects in the descendants of exposed parents–had been already detected in the 1920s by Herman Joseph Muller. He exposed fruit flies–drosophila–to X-rays and found malformations and other disorders in the following generations. He concluded from his investigations that low dose exposure, and therefore even natural background radiation, is mutagenic and there is no harmless dose range for heritable effects or for cancer induction. His work was honoured by the Nobel Prize for medicine in 1946. In the 1950s Muller warned about the effects on the human genetic pool caused by the production of low level radioactive contamination from atmospheric tests [1].
The International Commission on Radiological Protection (ICRP) recently decreased its risk estimate for heritable damage in 2007 [2,3]. Its Detriment Adjusted Nominal Risk Coefficient for radiation heritable effects in an exposed population was reduced from the previous 1990 value of 1.3% Sv-1 to 0.2% Sv-1 a greater than 6-fold reduction. The ICRP approach is based on a linear relation between dose and end-point, measured as heritable disease at or before birth. Evidence and arguments which we will present suggest that this linear assumption is invalid and that the ICRP value is unsafe when applied to the chronic low dose internal exposure range.
The belief that heritable consequences of radiation were negligible followed from studies of the Japanese survivors of the atomic bomb (A-bomb) explosions in Hiroshima and Nagasaki in 1945. The American-Japanese Institute in Hiroshima, Atomic Bomb Casualty Commission (ABCC), did not apparently find mutations in the descendants of the survivors. Therefore the ICRP derive its current risk figure from experiments in mice. The result corresponds to the evaluation by the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR committee) [4].
We will show that the current model for genetic effects of exposure is unsound and we present a more realistic one based on data. We will begin by pointing to some serious problems with the ABCC studies of genetic effects in the A-bomb survivors. These may be classed under four Error Types.
Type 1. The dose response problem. For genetic damage, increasing dose will not linearly increase effects since at high doses there will be sterility or fetal loss [5].
Type 2. The external/internal problem. The dose of interest is the energy delivered to the germ cells and their precursors. This may be much higher for internal radionuclides with affinity for DNA (strontium-90 [Sr-90], barium-140, uranium) [6].
Type 3. The philosophical method problem. If data is interpreted though a particular scientific model, evidence which cannot fit the model will be ignored, dismissed or invisible [7,8].
Type 4. Bias in the analysis of or presentation of data from the ABCC results. There have been a number of serious criticisms of the ABCC and later studies of cancer effects. The genetic studies were criticised by De Bellefeuille [9] who demonstrated the existence of significant genetic effects including sex-ratio and malformations which had been “lost” through the choice of analysis. However, De Bellefeuille’s observations were ignored by the risk agencies. The issue will be returned to in the discussion section.
Together these raise major doubts over the belief, expressed in ICRP103, Appendix B.2.01 [2], that “Radiation induced heritable disease has not been demonstrated in human populations.”
Effects in populations exposed to Chernobyl fallout are excluded by the official committees, which claim that doses are too low to generate statistically observable increases (the philosophical method problem: Error Type 3). This, however, is certainly wrong, because we know from many studies of chromosome aberrations, either that the doses calculated by UNSCEAR are much too low or that there is an enhanced radiobiological effectiveness (RBE) in the type of internal exposures or chronic delivery received by the Chernobyl groups. In other words, the biological or genetic damage from unit internal dose e.g., from a radioactive atom bound to DNA is far greater than for the same dose delivered externally. This is Error Type 2: internal/external problem. The doses upon which the ICRP risks are based, either from humans or mice, are external doses. There are significant issues regarding the equivalence for causing genetic damage of internal and external dose calculations [6]. Internal exposure to uranium by inhalation, for example, has been associated with significantly high genotoxicity resulting in anomalously high excess levels of chromosome damage and birth defects in a number of different groups [10]. Uranium binds to DNA, a fact that has been known since the 1960s [11–13]. Other group II calcium mimics and DNA seekers include the nuclide Sr-90 which causes significant genetic effects [14–17]. All epidemiological studies of radiation and health which define risk factors have been subject of this Error Type 2: external/internal problem, and have generally also defined risk in terms of cumulative integrated equivalent dose, and so real effects have been ignored or dismissed, the Error Type 3: philosophical problem.
Findings in Children Born After the Chernobyl Accident and in Kazakhstan
We previously published findings about fetal deaths, perinatal mortality and congenital malformations (CM) after Chernobyl [18]. Table 1 shows results for CM after Chernobyl. These appeared not only in the area of the exploded reactor but also in Turkey, Bulgaria, Croatia, and Germany. Our criteria for inclusion of this evidence was originally to present only observations which disagreed with the current ICRP/UNSCEAR paradigm but following questions by a reviewer we include discussion of one of the few studies with contemporary data which claims to have shown that there were no measurable heritable effects [19].
Table 1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4870760/table/t1-eht-31-e2016001/
Increase of congenital malformations after exposure by the Chernobyl accident
The EUROCAT Europe-wide Study
The study of Dolk and Nichols [19] is widely cited as evidence for no effect. The authors examined Down’s syndrome, neural tube defects (NTD), microcephaly, hydrocephaly, anopthalmos and congenital cataract in 16 EUROCAT registers. There were 231401 births in the areas in 1986. The 16 registries were divided into three groups of high (200 to 800 μSv), medium (97 to 190 μSv) and low (29 to 55 μSv). Three comparison cohort periods were defined as E (conception May 1986), T (conception May 1986 to April 1987 contains E), and C (control: conception May 1987 to April 1989). Authors concluded “no evidence of a generalised detectable increase in the prevalence of congenital anomalies in the first month or first year following Chernobyl.” But the choice of the cohort periods for a study of “heritable effects” is interesting. On the basis of whole body monitoring results, genetic damage to the germ cells from internal exposures will have continued well into the control period C and damage will have been cumulative [44]. We have reanalysed their data for combined NTD hydrocephaly, microcephaly and anopthalmia in all their exposure groups using their periods. A test of T vs. C cohorts showed a significant effect with odds ratio (OR) of 1.20 (95% confidence interval [CI], 1.02 to 1.4; p=0.014). This was apparent in the test of E vs. C though the numbers were smaller. However, there was no increasing monotonic relation between assumed “dose” category and effect and this clearly influenced the authors’ conclusions. This is the common response to the finding of high risks at low doses and represents a good example of the Error Type 1 referred to above. It appears that the results actually show an increased risk if we combine all the exposure levels.
Chernobyl Effects in Belarus
Belarus received most contamination from Chernobyl. A central registry for CM existed from 1979 and rates of CM before and after the Chernobyl accident could thus be compared. A number of studies are listed in Table 1. Comparison of legal abortuses in 1982 to 1985 and 1987 to 1994 showed combined CM increases of 81%, 49%, and 43% in regions of high (>555 kBq/m2), medium (>37 kBq/m2), and low (<37 kBq/m2) contamination, the effect being significant at the 0.05 level in all three [22]. The genetic origin is confirmed in those anomalies which are combined with a recognized mutation that is not present in either of the parents [18].
A study [23] confirmed the CM excess in the Strict Registration of Malformations System finding 86% increase in 1987 to 1996 vs. 1982 to 1985 (high contamination) and 59% (control regions) (p<0.05). The same authors reported significant excess chromosome aberrations of dicentric and centric rings rates of 0.39±0.09% (n=91) in Gomel and Mogilev (>555 kBq/m2) compared with a control region of Minsk, Grodno and Novopolotsk (<37 kBq/m2) (n=118; CM=0.09±0.04) [23].
To 2004 there was no decrease in these rates [45]. The authors think these effects are genetically induced because it is not plausible that doses in pregnant females rose in the period of decreasing environmental contamination and decreasing food contamination after the accident. A Belarussian-Israeli group [46] found the following increased polygenetic disease rates in children of Chernobyl- exposed parents: hematological diseases (6-fold), endocrine diseases (2-fold), diseases of digestive organs (1.7-fold).
A 1994 study compared Gomel (high exposure) with Vitebsk (presumed low exposure) for mortality in children zero to four finding absolute CM rates of 4.1% vs. 3%, respectively [24]. Savchenko [25] writing for the United Nations reported frequency of CM in regions of Gomel between 1982 to 1985 and 1987 to 1989 ranging from 170% in Dobrush to 680% in Chechersk.
Petrova et al. [27] compared two high and two low contaminated regions of Belarus for a number of indicators of pregnancy outcome and child health. For CM, before and after Chernobyl increases for all CM were: Gomel 150%>Mogilev 130%>Brest 120%>Vitebsk 110%, the rank of their contamination levels. Kulakov et al. [26] examined 688 pregnancies and 7000 births in Chechersky (Gomel, Belarus) and Polessky (Kiev, Ukraine). Sharp reductions in birth rates in both regions after Chernobyl were ascribed partly to abortions. High perinatal mortality was ascribed partly to congenital malformations. Incidence increased by a factor of two following the accident for congenital heart disease, esophageal atresia, anencephaly, hydrocephaly and multiple malformations. Total number of neonatal disorders increased in Polessky (Ukraine) from 1983 to 1985 to 1986 to 1990 from 6.81 to 21.32 (313%) and in Chechersky from 5.15 to 10.49 [26].
Chernobyl Effects in Ukraine
The studies by Wertelecki and colleagues [29,30] were valuable for quantifying the effects. The Pripyat region of Ukraine on the border of Belarus was significantly contaminated. Populations are dependent on local produce. Internal contamination was quantified for two groups, a high and lower dose group by whole body monitoring for caesium-137 (Cs-137). In addition, local produce was analysed for both Cs-137 and the DNA seeking Sr-90. The Sr-90/Cs-137 ratio was between 0.5 and two, so Sr-90 (with its DNA affinity and anomalous RBE) represented a significant internal exposure.
Other Reports of Chernobyl Effects on Birth Defects; Soviet Nuclear Test Site
Down´s syndrome as a certain genetic effect increased in several contaminated European countries [18,48]. An example is shown in Figure 1. In West Berlin, which was a kind of closed island at that time, the geneticist Sperling registered a sharp and significant increase in cases exactly nine months after the accident, also in Belarus [49]. UNSCEAR [4,20] dismissed these findings (and similar reports from Scotland and Sweden) on the basis that the doses were “below background.” The EUROCAT combined registry study [19] did not find an increase in Down’s syndrome, neither in the authors’ analysis nor in our reanalysis. Other evidence is presented in Table 1 of increased CM rates after Chernobyl in Germany, Turkey, Croatia and Bulgaria [21,32–37,50].

Congenital effects were found near the former Soviet nuclear test site in Kazakhstan near Semipalatinsk. Sviatova et al. [51] studied CM in three generations of inhabitants, investigating births between 1967 and 1997. They found significantly increased rates of CM combined, including Down’s syndrome, microcephaly and multiple malformations in the same individual.
Hereditary Effects in Children of Exposed Mothers
If a population is exposed, genetic effects will occur in the gonads of mothers as well as of fathers. A German investigation of occupationally exposed females showed a 3.2-fold significant increase in congenital abnormalities, including malformations, in offspring [52]. The authors interpret the effect as generated in utero but do not prove such a connection. In our opinion, this appears to be improbable given the short sensitive phase in pregnancy and the ban on pregnant females working in high risk environments.
The findings confirm early results in the Department of Medical Genetics of Montreal Children’s Hospital where the genetic effects of diagnostic X-rays were investigated [53]. The author observed the offspring of mothers who had been treated in childhood for congenital hip dysplasia since 1925 and were X-rayed for several times in the pelvic region. The ovarian dose was estimated to lie between 60 mSv to 200 mSv. In 201 living births of these females there were 15 individuals with severe malformations and other congenital distortions or Down’s syndrome and 11 cases with other abnormalities (all congenital abnormalities 12.9%) while the control group showed less than half of this rate. The latter was chosen from a large group of descendants where the parents were unexposed siblings of the study group.
Taken together with other evidence from sex-ratio (discussed below) these studies indicate that hereditary effects exist in the children of exposed mothers.
Findings in the Descendants of Occupationally Exposed Men Including Nuclear Test Veterans
Congenital Malformations
Studies in children of exposed men where the mothers were not exposed will show definite hereditary effects. A compilation of results for CM in offspring of exposed fathers is given in Table 2.
Table 2. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4870760/table/t2-eht-31-e2016001/
Congenital anomalies, especially malformations, in descendants (1st generationa) of occupationally exposed men
The anomalies seen in the descendants of Chernobyl liquidators (Nos. 5-7) also indicate unexpectedly high radiation sensitivity.
Three studies of nuclear test veterans have shown large increases in congenital effects in children and one study has found similar levels of congenital conditions in the grandchildren (Nos. 8-10). The British carried out nuclear weapon tests and activities in Australia (Maralinga) and Christmas Island in the Pacific between 1952 and 1967. More than 20000 young national servicemen and other military personnel were stationed at the test sites. The sites were contaminated with fission fallout and nanoparticles of uranium and plutonium from the weapons, tritium and carbon-14. Urquhart [61] analysed data in children from 1147 veteran families. Two hundred and thirty-three out of them had illnesses or defects (cancer, malformations, mental retardation) that could have a genetic origin: one in five families. They registered a 7:1 rate of abnormal children conceived before the tests vs. those conceived after the tests.
Two further studies of the offspring of a group of veterans have been published. Roff [62] carried out a questionnaire study of members of the British Nuclear Test Veteran Association (BNTVA) and reported excess rates of cardiovascular disorders, spina bifida, hydrocephalus and hip deformities. Busby and de Messieres [63] examined a different sample of the BNTVA, employed controls and compared with the European EUROCAT rates. Based on 605 veteran children and 749 grandchildren compared with 311 control children and 408 control grandchildren there were significant excess levels of miscarriages, stillbirths, infant mortality and congenital illnesses in the veterans’ children relative both to control children and expected numbers. There were 105 miscarriages in veteran’s wives compared with 18 in controls (OR, 2.75; 95% CI, 1.56 to 4.91; p<0.001). There were 16 stillbirths; three in controls (OR, 2.70; 95% CI, 0.73 to 11.72; p=0.13). Perinatal mortality OR was 4.3 (95% CI, 1.22 to 17.9; p=0.01) on 25 deaths in veteran children. Fifty-seven veteran children had congenital conditions vs. three control children (OR, 9.77; 95% CI, 2.92 to 39.3; p<0.001) these rates being also about eight times those expected on the basis of UK EUROCAT data for 1980 to 2000. For grandchildren similar levels of congenital illness were reported with 46 veteran grandchildren compared with three controls (OR, 8.35; 95% CI, 2.48 to 33.8; p<0.001).
Cancer and Leukemia
In 1984, an exceptionally high level of leukaemia cases in children and juveniles was reported in Seascale, near the nuclear reprocessing plant in Sellafield in Cumbria, UK. The authors explained this as a hereditary effect, because the fathers of the patients had worked in the plant [64]. The authorities argued that the doses were too low. The effect, however, had been described in principle already in experimental studies [65], and also after X-ray diagnostic exposures (Table 3). A significant number of other child leukemia and cancer studies have been carried out and are listed in Table 3.
Table 3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4870760/table/t3-eht-31-e2016001/
Cancer in children after preconceptional low-dose exposure of parents
The research of Hicks et al. [66] concerned exposed servicemen (Table 3). McKinney et al. [67] found a 3.2-fold increase in leukaemia and lymphomas in children of occupationally exposed men in three British regions in a case-control study.
Sex-ratio and X-linked Lethal Factors
Normally, it is not possible to study how many inseminated oocytes (zygotes) will be aborted after irradiation of the gonadal cells in humans. But it is observed that males who were exposed have fewer daughters than sons i.e., the male/female sex-ratio increases with dose.
Gene mutations may be responsible for the death of the zygote and will also occur in the sex chromosomes where they will predominantly affect the greater X-chromosome which can only be transmitted to a daughter. A dominant lethal factor will then lead to the death of the female zygote. Recessive lethal factors in the X-chromosome are much more frequent than dominant ones [74]. They affect only female births.
An impressive result was obtained in workers of the British nuclear fuel reprocessing plant at Sellafield in West Cumbria [75]. The county sex-ratio was 1055 boys/1000 girls, the normal value. For the children of fathers employed at Sellafield the ratio was 1094. For those with recorded doses greater than 10 mSv in the 90 days preconception period it was 1396, significant at the p<0.01 level. A similar effect was detected in cardiologists, who undertook interventional angiographic procedures involving X-ray exposures [76].
Scherb and Voigt studied different groups of inhabitants in a variety of countries after the Chernobyl accident for hereditary effects and found radiation-induced foetal deaths and early mortality, Down’s syndrome and alterations of the birth sex-ratio. They examined nuclear tests above ground which affected US inhabitants, Chernobyl emissions in Europe, and those living near German and Swiss nuclear plants. Results showed significant reduction in the female birth rate in all these [77,78].
The ABCC studies overall involve all the types of research error listed in the introduction, which we believe is the explanation for the failure to see excess heritable damage. The main problem was choice of controls. The sex-ratio studies were abandoned due to seemingly anomalous effects. De Bellefeuille [9] re-examined the issue in 1961 and found that results were biased by employing sex-ratios of children of parents who had both been exposed. Any effects, being in opposite directions, would therefore cancel out; his re-analysis based on children with only one exposed parent showed a clear effect in the expected direction. Padmanabhan [79] recently re-examined the issue using the original controls (abandoned by ABCC). Using the two not in city (NIC) groups Padmanabhan showed significant sex-ratio effects in the expected directions.
Sex-ratio is a very relevant parameter. It shows that genetic alterations are induced in the germ cells of males by very low doses, and it proves to be a sensitive indicator for exposures of the population.
Atmospheric Weapons test Fallout
The most significant global incident in terms of human exposure has been the atmospheric nuclear testing fallout which peaked between 1959 and 1963. It was this testing which worried Muller [1]. The tests increased the rates of neonatal and infant mortality in the US and the UK [80,81]. An interesting insight comes from a Canadian study of CM during the fallout period. le Vann [82] was concerned to examine the link between congenital malformation and the use of the drug thalidomide. He found that in Alberta there was no relation between the use of thalidomide and congenital birth outcomes but noted a strong association with precipitation; areas with high radioactive fallout had high levels of birth defects. Whilst we are not alleging that thalidomide does not have teratogenic effects, since many females in the le Vann study who never took any drugs gave birth to the typical “thalidomide spectrum” babies it seems that exposure to the fallout may have, as Muller [1] feared, have caused an effect. Ignoring this and the infant mortality findings involved a Error Type 3.
Genetic vs. Genomic, Mendelian vs. In Utero
We have not distinguished between Mendelian genetic effects involving the transfer of specific gene mutations to the offspring and effects consequent upon the operation of genomic instability, whereby the offspring inherit a tendency to apparently increase rates of all mutation above the normal rate for that population [83]. For the purposes of the arguments relating to radiation risk of harmful heritable conditions in the first generation such a discussion is unnecessary but needs to be revisited if multi-generational effects are being discussed. The question of germ cell damage in parents vs. in utero damage to development, though important, seems to us to be beside the point. All these CM effects are caused by mutation of DNA whether in the parental germ cells and precursors or from implantation to birth. Our aim is to assess the genetic risk based on observations. However, from the sex-ratio results it would seem that parental exposure is a dominant cause of radiation induced CM.
How Is It That the ICRP Risk Coefficient Is Wrong?
A reviewer asked us to address this question and to provide a brief account of biological mechanism. We begin with mechanism. The ICRP risk model is based on two big ideas: absorbeddose, which is average energy per unit mass of tissue, and the linear no threshold (LNT) response. For internal exposure to substances like Sr-90 and uranium, which both have high affinity for DNA, the concept of dose is meaningless [loc.cit. 6,10]. For CM as an outcome, it is also clear that the LNT model is unsustainable [5], because as the “dose” is increased from zero there are many blocks to the successful journey from germ cell to infant, the CM end point. Biological plausibility would predict an increase in damage and thus CM at very low dose, followed by a drop in CM due to failure to implant, early miscarriage, abortion. This would result in a saturation or “hogs-back” dose response in the lowest dose region. Only the survivors would make it to be registered as CM. The dose response would look like that in Figure 2 where A is the initial outcome and B is where the foetus dies or there is no implantation. The region C would relate to in utero effects later in gestation. There would be a fall in birth rate associated with region B and C; there usually is. You can see this effect most clearly in the EUROCAT studies where relative risk rises and then falls as dose increases [19]. It is perfectly clear in many other studies. It is clear in in analysis of infant leukemia after Chernobyl in 5 countries shown in Figure 3 [84] and the study of cleft palate in Bavaria [38,39] analysed by Korblein [40].


What Is the Correct Risk Coefficient?
The Chernobyl studies presented in Table 1 may be used to obtain an approximate risk factor for all CM in those exposed to fission spectrum radionuclides as assessed by Cs-137 area contamination. We can employ the data from Wertelecki et al. [30] on internal contamination to assess doses from Cs-137 and Sr- 90. The excess relative risk (ERR) for all CM follows a “hogsback” shaped response and is about 0.5 per mSv at 1 mSv saturating at between 0.1 to 0.2 per mSv at 10 mSv based on cumulative dose as assessed by ICRP models using Cs-137 area contamination as a basis of calculations. This means that the background rate will double or treble up to 10 mSv exposure and thereafter flatten out or fall. But it also results in a 50% excess risk at doses as low as 1 mSv. This ERR and dose response model accommodates all the observational data from Chernobyl and also elsewhere. We must make it clear that this model is for mixed internal and external exposure to fission product contamination doses as employed by UN agencies and may not necessarily apply to pure external exposures (e.g., X-rays, gamma- rays). However, it should be noted that Stewart’s finding of a 40% excess risk of childhood leukemia after a 10 mSv obstetric X-ray dose [71] is comparable with what is found at these higher doses in this review.
Conclusion
Genetically induced malformations, cancers, and numerous other health effects in the children of populations who were exposed to low doses of ionizing radiation have been unequivocally demonstrated in scientific investigations. Using data from Chernobyl effects we find a new ERR for CM of 0.5 per mSv at 1 mSv falling to 0.1 per mSv at 10 mSv exposure and thereafter remaining roughly constant. This is for mixed fission products as defined though external exposure to Cs-137. Results show that current radiation risk models fail to predict or explain the many observations and should be abandoned. Further research and analysis of previous data is suggested, but prior assumptions of linear dose response, assumptions that internal exposures can be modelled using external risk factors, that chronic and acute exposures give comparable risks and finally dependence on interpretations of the high dose ABCC studies are all seen to be unsafe procedures.
Acknowledgments
We are grateful to Marvin Resnikoff and Rick Haaker for running the Microshield program for dose rates over contaminated areas.
Footnotes
The authors have no conflicts of interest associated with material presented in this paper.
References
1. Muller HJ. Radiation damage to the genetic material. Am Sci. 1950;38(1):33–59. [PubMed]
2. International Commission on Radiological Protection The 2007 recommendations of the International Commission on Radiological Protection. 2007 [cited 2016 Jan 28]. Available from: http://www.icrp.org/publication.asp?id=ICRP%20Publication%20103.
3. International Commission on Radiological Protection 1990 Recommendations of the International Commission on Radiological Protection. 1991 [cited 2016 Jan 28]. Available from: http://www.icrp.org/publication.asp?id=icrp%20publication%2060.
4. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) UNSCEAR 2001 report: hereditary effects of radiation. 1991 [cited 2016 Jan 28]. Available from: http://www.unscear.org/unscear/en/publications/2001.html.
5. Doll R. Hazards of the first nine months: an epidemiologist’s nightmare. J Ir Med Assoc. 1973;66(5):117–126. [PubMed]
6. Busby C. Aspects of DNA damage from internal radionuclides. 2013 [cited 2016 Jan 28]. Available from: http://www.intechopen.com/books/new-research-directions-in-dna-repair/aspects-ofdna-damage-from-internal-radionuclides.
7. Platt JR. Strong inference: certain systematic methods of scientific thinking may produce much more rapid progress than others. Science. 1964;146(3642):347–353. [PubMed]
8. Feyerabend P. Against method. 4th ed. London: Verso; 2010. pp. 13–48.
9. De Bellefeuille P. Genetic hazards of radiation to man. I. Acta Radiol. 1961;56:65–80. [PubMed]
10. Busby C. Uranium epidemiology. Jacobs J Epidemiol Prev Med. 2015;1(2):009.
11. Huxley HE, Zubay G. Preferential staining of nucleic acid-containing structures for electron microscopy. J Biophys Biochem Cytol. 1961;11:273–296. [PMC free article] [PubMed]
12. Constantinescu DG, Hatieganu E. Metachromasia through uranyl ions: a procedure for identifying the nucleic acids and the nucleotides. Anal Biochem. 1974;62(2):584–587. [PubMed]
13. Nielsen PE, Hiort C, Sonnichsen SH, Buchardt O, Dahl O, Norden B. DNA binding and photocleavage by uranyl(VI)(UO22+) salts. J Am Chem Soc. 1992;114(13):4967–4975.
14. Luning KG, Frolen H, Nelson A, Ronnback C. Genetic effects of strontium-90 injected into male mice. Nature. 1963;197:304–305. [PubMed]
15. Ehrenberg L, Eriksson G. The dose dependence of mutation rates in the rad range, in the light of experiments with higher plants. Acta Radiol Diagn (Stockh) 1966;Suppl 254:73–78. [PubMed]
16. Stokke T, Oftedal P, Pappas A. Effects of small doses of radioactive strontium on the rat bone marrow. Acta Radiol Ther Phys Biol. 1968;7(5):321–329. [PubMed]
17. Smirnova EI, Lyaginskaya AM. Effects of small doses of radioactive strontium on the rat bone marrow. In: Moskalev YI, Idz Y, editors. Radioactive isotopes and the body. Moscow: Izdatel’stvo Meditsina; 1969. p. 348. (Russian)
18. Busby C, Lengfelder E, Pflugbeil S, Schmitz-Feuerhake I. The evidence of radiation effects in embryos and fetuses exposed to Chernobyl fallout and the question of dose response. Med Confl Surviv. 2009;25(1):20–40. [PubMed]
19. Dolk H, Nichols R. Evaluation of the impact of Chernobyl on the prevalence of congenital anomalies in 16 regions of Europe. Int J Epidemiol. 1999;228(5):941–948. [PubMed]
20. United Nations Scientific Committee on the Effects of Atomic Radiation UNSCEAR 2006 report vol. I: effects of ionizing radiation. [cited 2016 Jan 28]. Available from: http://www.unscear.org/unscear/en/publications/2006_1.html.
21. Hoffmann W. Fallout from the Chernobyl nuclear disaster and congenital malformations in Europe. Arch Environ Health. 2001;56(6):478–484. [PubMed]
22. Lazjuk GI, Nikolaev DL, Novikova IV. Changes in registered congenital anomalies in the Republic of Belarus after the Chernobyl accident. Stem Cells. 1997;2:255–260. [PubMed]
23. Feshchenko SP, Schröder HC, Müller WE, Lazjuk GI. Congenital malformations among newborns and developmental abnormalities among human embryos in Belarus after Chernobyl accident. Cell Mol Biol (Noisy-le-grand) 2002;48(4):423–426. [PubMed]
24. Bogdanovich IP. Medicobiological effects and the ways of overcoming the Chernobyl accident consequence. Minsk-Vitebsk: Ministry of Emergency and Chernobyl Problems of Belarus and Academy of Sciences of Belarus; 1997. Comparative analysis of the death rate of children, aged 0-5, in 1994 in radiocontaminated and conventionally clean areas of Belarus; p. 4. (Russian)
25. Savchenko VK. The ecology of the Chernobyl catastrophe: scientific outlines of an International Programme of Collaborative Research. Paris: United Nations Educational Scientific and Organisation; 1995. p. 83.
26. Kulakov VI, Sokur TN, Volobuev AI, Tzibulskaya IS, Malisheva VA, Zikin BI, et al. Female reproductive function in areas affected by radiation after the Chernobyl power station accident. Environ Health Perspect. 1993;2:117–123. [PMC free article] [PubMed]
27. Petrova A, Gnedko T, Maistrova I, Zafranskaya M, Dainiak N. Morbidity in a large cohort study of children born to mothers exposed to radiation from Chernobyl. Stem Cells. 1997;2:141–150. [PubMed]
28. Shidlovskii PR. General morbidity of the population in districts of the Brest region. Zdravoohranenie Belorussii (Minsk) 1992;1:8–11. (Russian)
29. Wertelecki W. Malformations in a Chernobyl-impacted region. Pediatrics. 2010;125(4):e836–e843. [PubMed]
30. Wertelecki W, Yevtushok L, Zymak-Zakutnia N, Wang B, Sosyniuk Z, Lapchenko S, et al. Blastopathies and microcephaly in a Chernobyl- impacted region of Ukraine. Congenit Anom (Kyoto) 2014;54(3):125–149. [PMC free article] [PubMed]
31. Godlevsky I, Nasvit O. Dynamics of health status of residents in the Lugyny district after the accident of the ChNPS. In: Imanaka T, editor. Research activities about the radiological consequences of the Chernobyl NPS accident and social activities to assist the sufferers by the accident. Osaka: Kyoto University Research Reactor Institute; 1998. pp. 149–156.
32. Akar N, Ata Y, Aytekin AF. Neural tube defects and Chernobyl? Paediatr Perinat Epidemiol. 1989;3(1):102–103. [PubMed]
33. Caglayan S, Kayhan B, Menteşoğlu S, Aksit S. Changing incidence of neural tube defects in Aegean Turkey. Paediatr Perinat Epidemiol. 1989;3(1):62–65. [PubMed]
34. Güvenc H, Uslu MA, Güvenc M, Ozekici U, Kocabay K, Bektaş S. Changing trend of neural tube defects in eastern Turkey. J Epidemiol Community Health. 1993;47(1):40–41. [PMC free article] [PubMed]
35. Mocan H, Bozkaya H, Mocan MZ, Furtun EM. Changing incidence of anencephaly in the eastern Black Sea region of Turkey and Chernobyl. Paediatr Perinat Epidemiol. 1990;4(3):264–268. [PubMed]
36. Moumdjiev N, Nedkova V, Christova V, Kostova S. Influence of the Chernobyl reactor accident on the child health in the region of Pleven, Bulgaria. International Pediatric Association. Excerpts from the 20th International Congress of Pediatrics; 1992 Sep 5-10; Rio de Janeiro, Brazil. Vevey: Nestlé Nutrition Services. 1992:57.
37. Kruslin B, Jukić S, Kos M, Simić G, Cviko A. Congenital anomalies of the central nervous system at autopsy in Croatia in the period before and after the Chernobyl accident. Acta Med Croatica. 1998;52(2):103–107. [PubMed]
38. Zieglowski V, Hemprich A. Facial cleft birth rate in former East Germany before and after the reactor accident in Chernobyl. Mund Kiefer Gesichtschir. 1999;3(4):195–199. (German) [PubMed]
39. Scherb H, Weigelt E. Cleft lip and cleft palate birth rate in Bavaria before and after the Chernobyl nuclear power plant accident. Mund Kiefer Gesichtschir. 2004;8(2):106–110. (German) [PubMed]
40. Korblein A. Abnormalities in Bavaria after Chernobyl. Strahlentelex. 2004;417:4–6. (German)
41. Government of Berlin West. Section of Health and Social Affairs . Annual health report. Berlin: Government of Berlin West; 1987. (German)
42. Lotz B, Haerting J, Schulze E. Changes in fetal and childhood autopsies in the region of Jena after the Chernobyl accident. 1996 [cited 2016 Jan 28]. Available from: http://www.meb.uni-bonn.de/gmds/abstracts/0095e.html (German)
43. Eckerman KF, Ryman JC. Federal guidance report 12: external exposure to radionuclides in air, water and soil. 1993 [cited 2016 Feb 20]. Available from: https://crpk.ornl.gov/documents/fgr12.pdf.
44. Busby C, Cato MS. Increases in leukemia in infants in Wales and Scotland following Chernobyl: evidence for errors in statutory risk estimates. Energy Environ. 2000;11(2):127–139.
45. Yablokov AV, Nesterenko VB, Nesterenko AV. Chernobyl– consequences of the Catastrophe for people and the environment. 2009 [cited 2016 Feb 20]. Available from: http://www.strahlentelex.de/Yablokov_Chernobyl_book.pdf. [PubMed]
46. Lomat L, Galburt G, Quastel MR, Polyakov S, Okeanov A, Rozin S. Incidence of childhood disease in Belarus associated with the Chernobyl accident. Environ Health Perspect. 1997;6:1529–1532. [PMC free article] [PubMed]
47. Scherb H, Sperling K. Today’s lessons from the Chernobyl accident. Naturwiss Rundsch. 2011;64(5):229–239. (German)
48. Sperling K, Neitzel H, Scherb H. Evidence for an increase in trisomy 21 (Down syndrome) in Europe after the Chernobyl reactor accident. Genet Epidemiol. 2012;36(1):48–55. [PubMed]
49. Zatsepin IO, Verger P, Gagniere B, Khmel RD, Belarus Institute for Hereditary Diseases Cluster of Down’s syndrome cases registered in January 1987 in Republic of Belarus as a possible effect of the Chernobyl accident. Int J Radiat Med. 2004;6(1-4):57–71.
50. Akar N. Further notes on neural tube defects and Chernobyl. Pediatr Perinatal Epidemiol. 1994;8:456–457. [PubMed]
51. Sviatova GS, Abil’dinova GZh, Berezina GM. Frequency, dynamics, and structure of congenital malformations in populations under longterm exposure to ionizing radiation. Genetika. 2001;37(12):1696–1704. (Russian) [PubMed]
52. Wiesel A, Spix C, Mergenthaler A, Queisser-Luft A. Maternal occupational exposure to ionizing radiation and birth defects. Radiat Environ Biophys. 2011;50(2):325–328. [PubMed]
53. Cox DW. An investigation of possible genetic damage in the offspring of women receiving multiple diagnostic pelvic X rays. Am J Hum Genet. 1964;16:214–230. [PMC free article] [PubMed]
54. Macht SH, Lawrence PS. National survey of congenital malformations resulting from exposure to roentgen radiation. Am J Roentgenol Radium Ther Nucl Med. 1955;73(3):442–466. [PubMed]
55. Sever LE, Gilbert ES, Hessol NA, McIntyre JM. A case-control study of congenital malformations and occupational exposure to low-level ionizing radiation. Am J Epidemiol. 1988;127(2):226–242. [PubMed]
56. Parker L, Pearce MS, Dickinson HO, Aitkin M, Craft AW. Stillbirths among offspring of male radiation workers at Sellafield nuclear reprocessing plant. Lancet. 1999;354(9188):1407–1414. [PubMed]
57. Shakhatreh FM. Reproductive health of male radiographers. Saudi Med J. 2001;22(2):150–152. [PubMed]
58. Tsyb AF, Souchkevitch GN, Lyasko LI, Artamonova YZ, Navolokin VV, Raykina LG. General characterization of health in first-generation offspring born to liquidators of the Chernobyl NPP accident consequences. Int J Radiat Med. 2004
59. Matveenko EG, Borovykova MP, Davydow GA. Physical characteristics and primary morbidity in liquidator´s children. In: Yablokov AV, Busby C, editors. Chernobyl 20 years after. Aberystwyth: Green Audit Books; 2006. pp. 176–179.
60. Liaginskaia AM, Tukov AR, Osipov VA, Ermalitskiĭ AP, Prokhorova ON. Congenital malformations among offspring of the liquidators of the consequences from Chernobyl accident. Radiats Biol Radioecol. 2009;49(6):694–702. (Russian) [PubMed]
61. Urquhart J. New Evaluation of Radiation Risk, International Conference of the Society for Radiation Protection. Bremen: Gesellschaft fur Strahlenschutz; 1992. Radiation exposure and subsequent health history of veterans and their children; pp. 209–216. (German)
62. Roff SR. Mortality and morbidity of members of the British Nuclear Tests Veterans Association and the New Zealand Nuclear Tests Veterans Association and their families. Med Confl Surviv. 1999;15 Supple 1:i-ix, 1-51. [PubMed]
63. Busby C, de Messieres ME. Miscarriages and congenital conditions in offspring of veterans of the British Nuclear Atmospheric Test Programme. Epidemiology (Sunnyvale) 2014;4:172.
64. Gardner MJ, Snee MP, Hall AJ, Powell CA, Downes S, Terrell JD. Results of case-control study of leukaemia and lymphoma among young people near Sellafield nuclear plant in West Cumbria. BMJ. 1990;300(6722):423–429. [PMC free article] [PubMed]
65. Nomura T. Parental exposure to x rays and chemicals induces heritable tumours and anomalies in mice. Nature. 1982;296(5857):575–577. [PubMed]
66. Hicks N, Zack M, Caldwell GG, Fernbach DJ, Falletta JM. Childhood cancer and occupational radiation exposure in parents. Cancer. 1984;53(8):1637–1643. [PubMed]
67. McKinney PA, Alexander FE, Cartwright RA, Parker L. Parental occupations of children with leukaemia in west Cumbria, north Humberside, and Gateshead. BMJ. 1991;302(6778):681–687. [PMC free article] [PubMed]
68. Graham S, Levin ML, Lilienfeld AM, Schuman LM, Gibson R, Dowd JE, et al. Preconception, intrauterine, and postnatal irradiation as related to leukemia. Natl Cancer Inst Monogr. 1966;19:347–371. [PubMed]
69. Shu XO, Gao YT, Brinton LA, Linet MS, Tu JT, Zheng W, et al. A population-based case-control study of childhood leukemia in Shanghai. Cancer. 1988;62(3):635–644. [PubMed]
70. Shu XO, Reaman GH, Lampkin B, Sather HN, Pendergrass TW, Robison LL. Association of paternal diagnostic X-ray exposure with risk of infant leukemia. Investigators of the Childrens Cancer Group. Cancer Epidemiol Biomarkers Prev. 1994;3(8):645–653. [PubMed]
71. Stewart A, Webb J, Hewitt D. A survey of childhood malignancies. Br Med J. 1958;1(5086):1495–1508. [PMC free article] [PubMed]
72. Natarajan N, Bross ID. Preconception radiation and leukemia. J Med. 1973;4(5):276–281. [PubMed]
73. Shiono PH, Chung CS, Myrianthopoulos NC. Preconception radiation, intrauterine diagnostic radiation, and childhood neoplasia. J Natl Cancer Inst. 1980;65(4):681–686. [PubMed]
74. Vogel F, Rohrborn G, Schleiermeyer E. Radiation genetics in mammals. Stuttgart: Verlag; 1969. (German)
75. Dickinson HO, Parker L, Binks K, Wakeford R, Smith J. The sex ratio of children in relation to paternal preconceptional radiation dose: a study in Cumbria, northern England. J Epidemiol Community Health. 1996;50(6):645–652. [PMC free article] [PubMed]
76. Choi JW, Mehrotra P, Macdonald LA, Klein LW, Linsky NM, Smith AM, et al. Sex proportion of offspring and exposure to radiation in male invasive cardiologists. Proc (Bayl Univ Med Cent) 2007;20(3):231–234. [PMC free article] [PubMed]
77. Scherb H, Voigt K. Trends in the human sex odds at birth in Europe and the Chernobyl Nuclear Power Plant accident. Reprod Toxicol. 2007;23(4):593–599. [PubMed]
78. Scherb H, Voigt K. The human sex odds at birth after the atmospheric atomic bomb tests, after Chernobyl, and in the vicinity of nuclear facilities. Environ Sci Pollut Res Int. 2011;18(5):697–707. [PubMed]
79. Padmanabhan VT. Sex ratio in A-bomb survivors. Evidence of radiation induced X-linked lethal mutations. In: Busby C, Busby J, Rietuma D, de Messieres M, editors. Fukushima and health: what to expect. Proceedings of the 3rd International Conference for the European Committee on Radiation Risk; 2009 May 5-6; Lesvos, Greece. Aberystwyth: Green Audit; 2012. pp. 273–304.
80. Sternglass EJ. Environmental radiation and human health. In: LeCam LM, Neyman J, Scott EL, editors. Proceedings of the Sixth Berkeley Symposium on Mathematical Statistics and Probability; 1971 Jul 19-22; Berkeley, CA, USA. Berkeley: University of Calififornia Press; 1971. pp. 145–221.
81. Whyte RK. First day neonatal mortality since 1935: re-examination of the Cross hypothesis. BMJ. 1992;304(6823):343–346. [PMC free article] [PubMed]
82. le Vann LJ. Congenital abnormalities in children born in Alberta during 1961: a survey and a hypothesis. Can Med Assoc J. 1963;89(3):120–126. [PMC free article] [PubMed]
83. Baverstock K, Belyakov OV. Some important questions connected with non-targeted effects. Mutat Res. 2010 [PubMed]
84. Busby CC. Very low dose fetal exposure to Chernobyl contamination resulted in increases in infant leukemia in Europe and raises questions about current radiation risk models. Int J Environ Res Public Health. 2009;6(12):3105–3114. [PMC free article] [PubMed]
New data show massive radiation levels in Odaka, Minamisoma
We are presenting here the most recent soil contamination map made by the “Environmental Radioactivity Measurement Project around Fukushima Daiichi Nuclear Power Plant.”


The area where measurements took place is shown by a green square in the map.
It includes two administrative units, Hanokura and Otomi of the Odaka district of Minamisoma town of Fukushima prefecture.

Here is the soil contamination map.

Taro Yamamoto of the Liberal Party, member of the House of Councilors, used another map prepared by the same group on two other administrative units of Odaka district during his questions at the Special Commission of Reconstruction of the House of Deputy on November 18th 2016.
We are quoting here some extracts of his questions *.
Taro YAMAMOTO
You are well aware of the existence of the Ordinance on Prevention of Ionizing Radiation Hazards. This is a rule that must be respected in order to protect workers exposed to risks related to ionizing radiation in establishments such as hospitals, research laboratories and nuclear power plants, isn’t it?
It contains the definition of the Radiation Control Zone. This is Article 3 of the Ordinance in File No. 1. It states that if the situation corresponds to the definition described in Article 3/1 or to that specified in Article 3/2, the zone shall be considered as a Radiation Control Zone and a sign must be posted there. I will read parts 1 and 2 of this article.
1: The area in which the total effective dose due to external radiation and that due to radioactive substances in the air is likely to exceed 1.3mSv per quarter – over a period of three months! When the dose reaches 1.3mSv over a period of three months, a zone is called a Radiation Control Zone.
Part 3/2 refers to the surface density in the attached table.
Here is File No. 2. What will it be if we do the conversion of the density of the surface per m2?
○ Government expert (Seiji Tanaka)
The conversion is 40,000Bq/m2
(…..)
In the town of Minamisoma in the coastal region of Fukushima Prefecture, three types of evacuation zones were established after the earthquake. In July 2016, the evacuation order was lifted in the “evacuation order lifting preparation area” and in the ‘’not-permitted-to-live area’’. There is only one household with two people remaining in the “the difficult-to-return-to area”.
According to the State, 90% of the territories of Minamisoma are safe.
There is a group called “The Measurement of Environmental Radioactivity Around the Fukushima Daiichi Nuclear Power Plant*** ” composed mainly of residents of Minamisoma. Since 2012, its members have been taking measurements of soil contamination in the vicinity of the members’ neighborhoods and in residential areas. They provided the information. Please take a look at File No. 3. You see a colored map.
This is the map of soil collected and measured in the territories where the decontamination works have been completed. The colors show the levels of contamination. The blue colored area indicates where the contamination measurements are below 40,000Bq / m2, ie below the level of a radioactivity controlled zone. There is only one, at the bottom right. Apart from this one, at all other places, the colors show measurements equivalent or higher than in a Radiation Control Zone. There is even an area colored gray where the measurements exceed 1,000,000Bq / m2. There are people living there!
END OF QUOTE
The evacuation order is already lifted from Odaka district of Minamisoma town, and officially the decontamination work has finished. However, the two maps show that in wide areas highly radioactive soil is being found. Their measurements are well above the lower contamination limit of a Radiation Control Zone.
In a Radiation Control Zone, following the Ordinance on Prevention of Ionizing Radiation Hazards, it is prohibited to drink, eat or stay overnight. Even adults are not allowed to stay more than 10 hours. To leave the zone, one has to go through a strict screening.
How can people live there?

The policy to make a population return and live in areas even more contaminated than most of the Radiation Control Zone, while cutting the financial and housing aid for evacuees, is a serious infringement of human rights.
___
* Source : Taro YAMAMOTO’s website
** Ordinance on Prevention of Ionizing Radiation Hazards, Ministry of Labour Ordinance No. 41 of September 30, 1972, Latest Amendments: Ministry of Health, Labour and Welfare Ordinance No. 172 of July 16, 2001
*** Fukuichi shûhen kankyôhôshasen monitoring project
ふくいち周辺環境放射線モニタリングプロジェクト (in Japanese)
Facebook
___
Read also…
Full English translation of Taro Yamamoto’s questions : “Taro Yamamoto defends Fukushima victims’ rights”
About activities of “Environmental radioactivity Measurement Project around Fukushima Daiichi Nuclear Power Plant”, read “Minamisoma Whistleblowers, Fukushima”
__
Thanks to Pierre Fetet and Hervé Courtois for providing the contamination map of Kanabuchi and Kanaya of the Odaka district.
https://fukushima311voices.wordpress.com/2017/01/12/new-data-show-massive-radiation-levels-in-minamisoma/
Gun control heartburn: Radioactive boars are amok in Fukushima

The “most adaptable animals that you’ll ever find” are running rampant across parts of rural Japan in the wake of the 2011 nuclear catastrophe and strict gun laws aren’t helping.
The Fukushima Daiichi nuclear disaster, in which a boiling water reactor nuclear power plant largely went Chernobyl after a tsunami knocked it offline has left Japan with a host of problems to include radiation-induced health impacts, some 200,000 displaced locals and possible exposure of groundwater to melted down nuclear fuel for decades to come.
Oh yeah, and the wild hogs.
According to an article in The Washington Post last April, the boar population, lacking natural predators is booming. Worse, thousands of the animals roam an area where highly radioactive caesium-137, which has a half-life of 30 years, has been confirmed.
Most agree that the best way to eradicate the rapid population of would-be Orcs is through hunting, but in gun control-friendly Japan, that is easier said than done.
“Something that complicates wild boar management in Japan is the exceptionally restrictive ownership, use, and access to firearms,” says Dr. Mark Smith, a forestry and wildlife professor at Auburn University, told Outside online. “This includes not only the general populace, but also with researchers, wildlife biologists, and natural resource managers.”
According to the Australian-based Small Arms Survey, the rate of private gun ownership in Japan is 0.6 per 100 people with only 77 handguns in circulation and just 0.8 percent of Japanese households containing one or more legal guns, most often shotguns.
Smith went to Japan to study the problem in 2013.
“Although [recreational] hunting does occur in Japan, it is very limited,” says Smith, “and hunter numbers are declining by the year, so there are fewer and fewer hunters out there harvesting wild boar.”
Plus there is the problem with the meat. In short, there is no good way to make caesium-137 infused pork a balanced part of your complete meal without the diner glowing in the dark, no matter how much BBQ sauce you use.
In Japan, they have to incinerate the carcasses (at 1,771 degrees Fahrenheit) then obliterate the fragments left over with hammers and box them up. Carefully.
Furthermore, the animals are very smart.
“They are the most adaptable animals that you’ll ever find: we call them the ‘opportunistic omnivore,’” says Smith.
http://www.guns.com/2017/01/03/gun-control-heartburn-radioactive-boars-are-amok-in-fukushima/
Contaminated Glove, Jacket, pants worn by a Fukushima Daiichi worker
By Marco Kaltofen
Activity is 0.7 to 240 kBq/kg, surface rad to 59 uR/hr.
http://bostonchemicaldata.com/data.html

35.5 kBq/kg

0.11 to 0.24 kBq/kg

ND (<0.01) to 17.1 kBq/kg
1 This Month
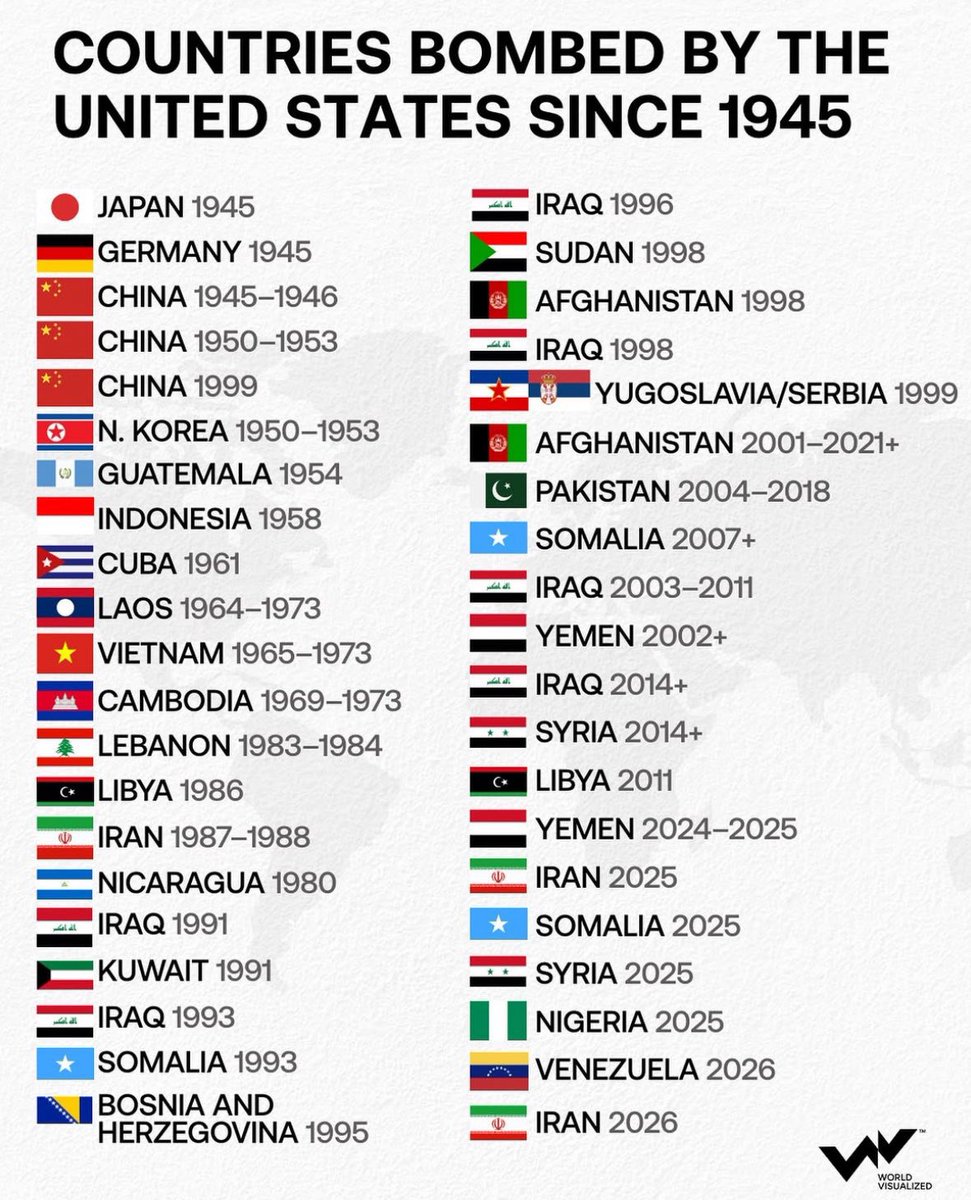
18 March Webinar @ 1 PM EST: An Assessment of SMR Projects: The Case of Canada
register for the zoom:
https://us02web.zoom.us/webinar/register/WN_o8BIIOUvQ2ONJR1nta65DQ#/registration

of the week – STOP SMALL MODULAR REACTORS IN CANADA
To see nuclear-related stories in greater depth and intensity – go to https://nuclearinformation.wordpress.com
-
Archives
- March 2026 (140)
- February 2026 (268)
- January 2026 (308)
- December 2025 (358)
- November 2025 (359)
- October 2025 (376)
- September 2025 (258)
- August 2025 (319)
- July 2025 (230)
- June 2025 (348)
- May 2025 (261)
- April 2025 (305)
-
Categories
- 1
- 1 NUCLEAR ISSUES
- business and costs
- climate change
- culture and arts
- ENERGY
- environment
- health
- history
- indigenous issues
- Legal
- marketing of nuclear
- media
- opposition to nuclear
- PERSONAL STORIES
- politics
- politics international
- Religion and ethics
- safety
- secrets,lies and civil liberties
- spinbuster
- technology
- Uranium
- wastes
- weapons and war
- Women
- 2 WORLD
- ACTION
- AFRICA
- Atrocities
- AUSTRALIA
- Christina's notes
- Christina's themes
- culture and arts
- Events
- Fuk 2022
- Fuk 2023
- Fukushima 2017
- Fukushima 2018
- fukushima 2019
- Fukushima 2020
- Fukushima 2021
- general
- global warming
- Humour (God we need it)
- Nuclear
- RARE EARTHS
- Reference
- resources – print
- Resources -audiovicual
- Weekly Newsletter
- World
- World Nuclear
- YouTube
-
RSS
Entries RSS
Comments RSS
